. SPOTS
ULTRASOUND BIOMICROSCOPY
[ Dec-05 ]
PRINCIPLES-
It is an imaging process which involves use of high frequency transducer to produce high resolution images of anterior segment structures.
Frequency- 50 MHz
Resolution- 60 microns
Depth perception- 4mm
TECHNIQUE-
INDICATIONS-
Anterior segment cysts & tumours
Pars planitis.Uveitis with miotic pupils
Cataract
Assessment of zonular integrity
Ant seg FB
Plateau iris
Post v’tomy VH
Unexplained hypotony
IOL malpositions
Failed filtering surg
Pigment dispersion syn
Pre-penetrating KP angle assessment
Malignant glaucoma
CONJUNCTIVAL PAPILLOMA-
PLATEAU IRIS SYN-
IOL COMPLICATIONS-
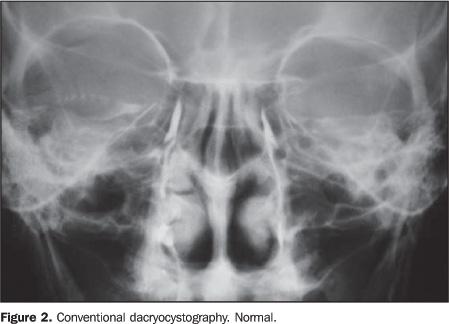
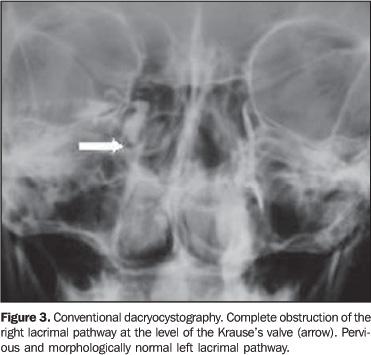
DACRYOCYSTOGRAPHY
Helpful in documenting functional & morphological status of tear flow by visualizing the true dimensions of the passages.
TYPES-
1.Plain DCG
2.Distention DCG
3.Macro DCG
4.cinematography
5. Dacryosintography
DYES-
Lipoidal in water / olive oil
Iodized oil
Neohydroil angiographin
Dionosil aqueous
Conray
Diagonal viscous
7. Ethiodized oil [0.5-1ml]
Viscous & water soluble contrast media stay well as well as spread well to give better contrast & do not hav globule formn
PLAIN DCG-
DISTENTION DCG-
Named so, bcos the passage is kept distended throughout the procedure of taking x-ray by pushing the radioopaque dye till x-rays are taken.
Water’s & lateral view
Adv over plain DCG-exact idea of the size of sac
-diverticula
-false passage
MACRO DCG-
Film cassette is kept under the x-ray table on a wooden stool.
Head of the pt is midway bet the x-ray tube & the film.
AP & lateral views
A set of delayed films taken after 15-30 min to see for partial obstrn
Adv-
Canalicular dis & obstrn are best seen by magnificatiom
Details enhanced by very good contrast
Small focus beam gives sharp image
CINEMATOGRAPHY-
DACRYOSINTIGRAPHY-
Non-invasive
Two drops of radiotracer Tc99m used in each eye
Series of images of both eyes taken at interval of 5 min for 35-40min by Gamma camera.
Appearance of tracer in nasal cavity noted.
Persistent pooling of radiotracer in lacrimal sac → obstrn at NLD-sac juncn
Also helps to diff epiphora d/t blockage from epiphora d/t lacrimal pump dysfunction
FLUORESCEIN ANGIOGRAPHY
DEF-
Involves photographic surveillance of the passage of fluorescein thru the retinal & choroidal circulation.
HISTORY-
Earliest description-1958- Chao & Flocks
Clin use-1961- Novotny & Alvis
PRINCIPLES-
FLUORESCENCE- It is the property of certain molecules to emit light energy of a longer wavelength wen stimulated by light of a shorter wavelength.
Excitation peak- 490 nm [ blue]
Represents the max absorption of light by fluorescein
Molecules stim by this wavelength will be excited to higher energy level & will emit light of a longer wavelength at 530nm [green]
FUNDUS CAMERA-
2 types of filters-
1. Blue excitation filter-
Thru this passes white light from the camera flash. The emerging blue light enters the eye & excites the fluorescein molecules in retinal & choroidal cir→Light of a longer wavelength is emitted [ yellow-green]
2.Yellow –green barrier filter-
Blocks any reflected blue light from the eye,allowing only yellow-green light to pass thru unimpeded to be recorded on film.
CHEMICAL PROPERTIES-
Orange water soluble dye
Chem. Related to phenolphthalein
Results from interaction of phthalic acid anhydride & resorcinol which in an alkaline sodium salt sol form sodium fluorescein [ C20 H10 O5Na2]
Low mol wt-367.27
High water solubility→ rapid diffusion
Absorption peak- 420-490nm
Emission peak- 510-530nm
Fluorescein binding- 70-85% -fluo bound
Remainder –free
Diffuses freely thru-choriocapillaries
-Bruch’s mem
-ON
-Sclera
-Ciliary Vs
-Ciliary body
* Does not diffuse thru-Retinal BVs
-RPE
-Large choroidal Vs
TECHNIQUE-
Adequate pupillary dilatation [6-8mm]
Pt is seated in front of fundus camera
Fluorescein, 5ml of 10 % [ 3ml of 25% -opaque media]
Red free photo taken
Fluo is injected rapidly into antecubiatal vein
After 5-25 sec, photo taken at 1 sec interval
After transit phase has been photographed in one eye,Control pictures of other eye are taken.If leakage is anticipated, late photo may be taken after 10 min.
ADVERSE EFFECTS-
Skin & urine discolouration
Nausea & vomiting
Flushing of skin, itching & hives
Dyschromatopsia
Phlebitis
Syncope,laryngeal edema , bronchospasm & anaphylactic shock.
PRECAUTION-
Avoid extravasation of dye to prevent tiss infiltration & tiss necrosis
C/I- Relative- 1st trim of pregnancy
ENTRY OF FLUO →
Dye enters the eye thru the Ophthalmic A.
Flu→ Short PCA→ choroidal cir
Flu→Central retinal A→ Retinal cir
As the route to retinal cir is longer than the choroidal cir, ret BVs fill 1 sec later than the choroidal cir.
PHASES-
Choroidal phase
Arterial phase
Arteriovenous phase
Venous phase
Late [Elimination phase]
1] CHOROIDAL PHASE-
* Rapid phase
* Dye reaches choroidal cir but not the ret As
* Occurs 8-12 sec after inj
* Patchy filling is d/t perfusion of choriocapillaries lobules sequentially rather than simultaneously.
* Visualisation of the choroid is k/as-‘Choroidal flush’
2. ARTERIAL PHASE-
* 0.5-1 sec after choroidal phase.
* Initially only the axial [midstream] segment of arterial bld fluoresces
* Bld plasma adjacent to the vessel wall stains later.
3.ARTERIOVENOUS PHASE-
* 1-2 sec after arterial phase
* Complete filling of arteries & capillaries & early laminar flow in the vein.
* Laminar flow is d/t rapid flow of plasma along the wall & higher conc of RBCs in central V lumen
4. VENOUS PHASE-
3 phases-
a) Early phase-3 sec after arterial phase
-complete arterial & capillary filling & more marked
Laminar venous flow
b) Mid-phase-Almost complete venous filling
c)Late phase- 5-20 sec after arterial filling
-complete venous filling & reduced conc in arteries
5.LATE [ELIMINATION] PHASE-
* With each succeeding wave,intensity of fluo becomes weaker
* Flu is absent from the angiogram after 5-10 min & totally eliminated from the body in sev hrs.
RETINAL CIRCULATION TIME-
Duration of time bet the first appearance of dye in the arterial cir upto its appear in tributary venous sys.
ARM TO RETINA TIME-
Time bet fluo inj & appear of dye in the eye [ optic disc ]
8.5-11 sec
Clinically FA of the disc is of greatest value in diff pseudopapilloedema [ drusen- optic n head & hyperopic disc] from papillitis & papilledema [same appear]
Exposed drusens- Autofluorescence
Buried drusens- hyperfluorescence d/t staining .NO LEAKAGE
Papilloedema- Hyperfluorescence & leakage
ABNORMAL FLUORESCENCE-
HYPERFLUORESCENCE-
Increased fluor d/t visualization of a nml quantity of fluo in the fundus or an absolute increase in the fluo content of the tissue.
TRANSMISSION / WINDOW DEFECT-
Drusen
Atrophy
Hereditary maculopathy
Toxic maculopathy
2.POOLING OF DYE- d/t breakdown of outer BRB-
→ Subretinal space- SRNVM
-CSR
→Sub-RPE Space- PED
3.STAINING OF TISSUE-
* Drusen
* Soft exud
* Scar tiss
* Vessel wall staining
4.LEAKAGE OF DYE-
- Abnormal choroidal vasculature→ Choroidal NV-Lacy pattern
- Abnormal disc / retinal vasculature→ PDR
-Breakdown of inner BRB→ CME-Petalloid appear
HYPOFLUORESCENCE-
Reduction / Absence of fluorescence
BLOCKAGE OF RETINAL FLUORESCENCE-
BLOCKAGE OF CHOROIDAL FLUORESCENCE-
-Sub-RPE / subretinal space- blood
-Choroidal lesions- neavi
-Increased density of RPE- Congenital hypertrophy of RPE
3.FILLING DEFECTS-
-Vascular occlusion- CRVO,
- CRAO
-BRVO
-Capillary dropout
- Loss of vascular bed- sev myopic degeneration
RETROFLUORESCENCE
Occurs when a non-fluoresent structure is silhouted against a background fluorescence.
FLUORESCEIN LEAKAGE-
Passage of dye beyond the physiologic barrier of the retinal V or RPE & spread into spaces bet cells or tiss layers.
FLUORESCEIN POOLING-
Leakage into anatomic space.
FLUORESCEIN STAINING-
Dye transiently attaches to tissues thereby causing fluorescence.
PSEUDOFLUORESCENCE-
AUTOFLUORESCENCE-
It is the innate property of fluorescence of certain ocular tiss like lens, BM [ Descemet’s memb, Bruch’s memb] & CB.
D/t lipofuschin
Eg- optic disc drusen
-Astrocytic hamartomas
VIVA-
Melanin
Lipofuschin
Avascularity of FAZ
Blockage of choroidal fluo by increased xanthophylls
Blockage of choroidal fluo by longer & thinner melanin
Inner BRB-Tight endothelial cell juncn of ret capillaries
Outer BRB- RPE cells [ zonula occludentes]
DARK CHOROID-
Atypical Stargardt’s dis
[ Typical Stargardt’s –pisciform speckles are hyperfluor]
Choroidal ischaemia
Argyrosis
INDOCYANINE GREEN
-98 % albumin bound→Reduces passage of ICG thru the fenestrations of choriocapillaries which are impermeable to albumin.
* Fluor is only 1/25th of fluorescein
Excitation peak- 805nm
Emission peak- 835nm [infrared spect]
-xanthophyll
-exud
-thin layers of subret bld
TECH-
ICG powder -40mg in 2ml
Pt seated in front of fundus camera
Red-free photo
Bet 25-40mg dye injected
Photo taken at 3min, 10min & 30min
Late phase yields the most useful informn as dye remains in the NV tiss after leaving ret & choroidal cir.
ADVERSE EFFECTS-
Staining of stools
Nausea & vomiting
Sneezing
Pruritis
C/I-
Pts allergic to iodine
pregnancy
PHASES-
EARLY PHASE-
2-60 sec
Hypofluo of optic disc
Poor perfusion of watershed zone
Prominent filling of choroidal As & early filling of choroidal veins
Retinal As are visible but not veins
EARLY MIDPHASE-
LATE MIDPHASE-
3-15min
Fading of choroidal V filling
Retinal Vs are still visible
Diffuse hyperfluor d/t diffusion of dye from choriocapillaries
LATE PHASE-
15-30 min
Hypofluo of choroidal vasculature against background hyperfluor
Lack of visibility of ret Vs
Dye remains in NV tiss after it has left chor & ret cir.
ABNORMAL FLUORESCENCE-
HYPERFLUORESCENCE-
RPE window defect
leakage from ret / choroidal cir or ONH
Abnml BVs
HYPOFLUORESCENCE-
Blockage of fluor- by bld, pigment, exud
Obstrn of cir
Loss of vascular tiss
RPE detachment [Hyperfluorescent on FA]
CORNEAL TOPOGRAPHY
For Cor topo images- my computer→ Anirban’s documents→my pictures
NORMAL CORNEA-
WITH-THE –RULE ASTIGMATISM-
Regular ast- steepest & flattest axes are at right angles to each other
With-the-rule Ast-Steepest axis is along the vertical meridian
Against-the-rule Ast-Steepest axis is along the horizontal meridian
Astigmatic pattern is k/as ‘’Bow-tie”
KERATOCONUS SUSPECT-
MILD KERATOCONUS-
MOD KERATOCONUS-
ADVANCED KERATOCONUS-
PELLUCID’S MARGINAL DEGENERATION-
Localised inferior peripheral steepening
Inferior crescent shaped ectasia with its horns curved centrally .
Flattening of vertical axis in the central cor [blue]
PTERYGIUM-
INTERPRETATION OF A COLOUR CODED MAP-
yellow & Green- Normal cornea
Hot colours- Red & its hues represent steep portions
Cool colours- Blue & its hues represents flat portions
SCALE-
ABSOLUTE SCALE-
Each colour represents a 1.5 D interval between 35 & 50 D , whereas above & below this range ,colours represent 5D interval.This scale is used in preoperative screening.
NORMALIZED SCALE-
Cornea is divided into 11 equal colours spanning the eye’s total diopteric power.
This scale gives more minute topographic details.
CLINICAL APPLICATIONS-
Early diagnoses of corneal dis-
Contact lens-
Routine CL [ rigid] fitting
Fitting in diff cases- post KP, keratoconus,postRK.
CL induced changes- central irreg astig, corneal warpage etc.
Keratoconus-
Depicted as a localized area of increased surface power surrounded by concentric zones of of decreased power.
Initial inv is in inferotemporal quad
MICROBIOLOGY
-Staph
-Strepto
-Moraxella
-Diphtheroids
STAINS-
GRAM STAIN-
Stain with crystal violet [blue-black]
Then iodine
Decolorize with acetone
Counterstain with carbol fuschin [red]
Gm +ve→ Resist decolouration & stain blue
Gm –ve→ Decolourize to pink / red
2.ZEIHL NEELSON STAIN-
* Stain with carbol fuschin
* Heat
* Decolourize with acid / alcohol
* Counterstain with Malachite green / methylene blue
GRAM +VE COCCI-
Staph aureus – coagulase +ve
_ aerobic
_ non-motile
_ non-sporing
Staph epidermidis-Aerobic
-non-motile
-non-sporing
Strepto pneum-encapsulated
-aerobic
-non-motile
-lyse RBC on agar ( alpha hemolysis)
Haemolysis- Partial- alpha- [ greenish]
-Complete- Beta- [colourless]
GRAM –VE COCCI-
Neisseria- diplococci
-aerobic
-non-motile
N. meningitides-Ferments glucose & maltose
N.gonorrhoea- Ferments only glucose
Growth- Thayer Martin med
GRAM +VE RODS-
Bacillus
Clostridium
Corynebacterium
Propionibacterium[ resides in meibomian glds]→ Endophthalmitis
GRAM –VE RODS/ BACILLI-
Pseudomonas-pyocin [green piment]
-aerobic
-non-motile
2. Haemophillus
3. Enterobactericiae- Grow on Mac conkey agar
-e.coli
-salmonella
-shigella
-proteus
-Klebsiella
-yersinia
4. Moraxella
FUNGUS-
Yeasts
Filamentous
Dimorphic
YEAST-
Candida
Cryptococc
FILAMENTOUS-
Aspergillus
Mucormycosis rhizopus
3.Fusarium
DIMORPHIC-
Blastomycosis
Coccidiodomycosis
Histoplasma
CULTURE MEDIA-
Staph aureus-
NUTRIENT AGAR-
Colonies-large,circular,convex,smooth,shiny,opaque
Golden yellow pigment
2.NUTRIENT AGAR SLOPE-
* Oil-paint appear
3. MAC CONKEY’S MEDIUM-
* Smaller colonies
* Pink d/t lactose fermentation
Streptococcus-
BLOOD AGAR-
Colonies- small,circular,semitransparent with clear hemolysis around them
Virulent strains- ‘matt’ colony
Avirulent strains- ‘glossy’ colony
Pneumococcus-
BLOOD AGAR-
colony- small, dome-shaped & glistening
area of greenish discolouration [haemolysis] around them,
AUTOMATED PERIMETRY [j-02]
DEF-
Perimetry involves evaluation of the visual field.
VISUAL FIELD-
Island of vision surrounded by a sea of darkness.
Limits-Superiorly- 60 deg
-Nasally- 60 deg
-Inferiorly- 70 deg
-Temporally- 90 deg
* Blind spot is located temporally bet 10 & 20deg.
-Represents the ONH.
ISOPTER-
Encloses an area within which a target of a given size is visible .
SCOTOMA-
An area of visual loss surrounded by vision.
ABSOLUTE SCOTOMA-
RELATIVE SCOTOMA-
Area of partial visual loss within which brighter & larger targets can be seen but smaller & dimmer ones cannot be seen.
LUMINANCE-
Intensity or brightness of light stimulus, measured in apostilbs [asb]
DIFFERENTIAL LIGHT SENSITIVITY-
The degree by which luminance of a target requires to exceed background luminance so as to be perceived by the eye.
TYPES OF PERIMETRY-
KINETIC PERIMETRY-
-Tangent screen
-Lister perimeter
-Goldman perimeter
STATIC PERIMETER-
3-dimensional assessment of the height of a pre-determined area of hill of vision
Presentation of a non-moving stimuli of varying luminance in the same pos to obtain a vertical boundary of the visual field.
Eg-Goldman’s peri
-Friedman’s peri
-Automated perimeter
SUPRATHRESHOLD STATIC PERIMETRY-
THRESHOLD PERIMETRY-
In Humphery’s perimeter, intensity of stim is increased by 4 db steps until threshold is crossed.Threshold is then redetermined by decreasing the intensity by 2 db steps. This is k/as –Bracketing.
SOURCES OF ERROR-
MIOSIS-Pupils less than 3mm shud be dilated
LENS OPACITIES-
UNCORRECTED REF ERROR-If a hyperopic person who usually wears contact lens is tested wearing spect→ magnify & enlarge the scotomas
SPECTACLES- Rim scotomas
5.PTOSIS- Suppresion of superior field
6.INADEQUATE RETINAL ADAPTATION- Leads to error if perimetry is performed soon after ophthalmoscopy.
HUMPHERY PERIMETRY-
The number before the dash (24- or 30-) indicates the area of the tested field in degrees from fixation
-The -2 strategy inv a grid of test points spaced 6 deg apart, offset from the vertical & horizontal meridian whereas the -1 strategy includes points along the vertical & horizontal meridian.
* RELIABILITY INDICES-
Reflect the extent to which patient’s results are reliable & shud be analysed first.
FIXATION LOSSES-
Indicates steadiness of gaze during the test
Heijl- Krakau method-Physiological blind spot is detected by presenting stim in the phy blind spot.If the pt responds, a fixation loss is recorded.
Shud be less than 20 %.
2.FALSE POSITIVES-
Stim is presented along with sound.
If sound alone is presented & pt responds→ False +ve→Trigger Happy pt
Shud not exceed 33%
Fields that show much larger defects in the pattern deviation plot than in the total deviation plot may be the result of high false positive errors.
3.FALSE NEGATIVES-
* Detected by presenting stim much brighter than threshold at a location where sensitivity has already been recorded.
* If the pt fails to respond→ False Neg
* Indicates- inattention
-Short term fluctuation
-disease severity
* Shud not exceed 33 %.
DISPLAYS-
GREYSCALE-
NUMERICAL DISPLAY-
Gives the threshold for all points checked
Figures in the bracket indicate threshold at the same point checked a second time,if on initial testing it was atleast 5 db less sensitive than expected.
TOTAL DEVIATION-
PATTERN DEVIATION-
PROBABILITY VALUES-
GLOBAL INDICES-
MEAN DEVIATION [MD]-
Measures overall field loss i.e. elevation or depression
2.PATTERN STANDARD DEVIATION [PSD]-
* Measure of focal loss or variability within the field taking into account any generalized depression in the hill of vision
* More specific indicator than MD.
3. SHORT TERM FLUCTUATION [SF]-
* Indicator of consistency of responses
* Threshold is measured twice at ten pre-selected points & calculated on the basis of diff bet 1st & 2nd measurement
* Shud nmlly be less than 2 db.
* > 3dB suggests unreliable or damaged field
4. CORRECTED PATTERN STANDARD DEVIATION [CPSD]-
* Measure of variability within the field after correcting for short term fluctuation.
GLAUCOMATOUS FIELD DEFECTS-
ARCUATE / BJERRUM’S AREA-
Arches above & below the fixation from the blindspot to the median raphe,corresponding to the arcuate retinal fib.
Early visual loss in glauc commonly occurs within this arcuate area, specially in the superior half which correlates with the predilection of the inferior & superior temporal poles of ONH for early glaucomatous damage.
DEFECTS-
BARING OF BLIND SPOT
PARACENTRAL SCOTOMA-
3.SEIDEL SCOTOMA-
- The paracentral scotomas elongate circumferentially along the arcuate nerve fib & connect with blind spot to form Seidel scotoma
4. NASAL ROENNE’S STEP-
Due to diff in sensitivity above & below the horizontal midline in the nasal field.
ARCUATE / BJERRUM SCOTOMA-
6.DOUBLE ARCUATE / RING SCOTOMA-
-Seen with further progression.
7. TEMPORAL & CENTRAL ISLAND OF VISION-
Temporal island extinguishes before the central.
Few important points-
Glaucomatous defects start in the central 30 deg of visual field.
Neurological defects are hemianopic i.e they respect the vertical meridian.
The dimmest stimulus that can be seen by a young , well-trained observer is about- 38-40db.
0db corresponds to the maximum brightness a perimeter can produce
Normal blind spot diameter- 6 degree
Normal testing distance of Humphery perimeter is 30 cm
If a large change is seen & part of field loss seems hemianopic or occurs in the other eye as well, neurological causes are generally the rule.
-Also k/as Blue-yellow perimetry
- Goldman size V stimuli of blue colour is presented on a bright yellow background
-The yellow background serves to reduce the responsiveness of the red & green cone systems so that the blue stimuli are primarily seen by the blue cone system only.
- SWAP is more sensitive than standard perimetry in detecting-
* Neuro-ophthalmic dis
* ARMD
* Migraine
* Diab macular edema
* OHT
-The defects are larger than those found with std perimetry
-Disadv- Lens absorbs blue light & so the field changes caused by absorption of light by the lens cannot be differentiated
GLAUCOMA HEMIFIELD TEST-
Gives information concerning differences bet the superior & inferior halves of the visual field by evaluating threshold at mirror image points above & below the horizontal meridian
NON-GLAUCOMATOUS FIELD DEFECTS-
Sec OA- Nasal field defect
Optic disc drusen- Arcuate defect
Chiasmal lesion- Bitemporal hemianopia
-Respect the midline
* Postchiasmal lesion-Homonymous hemianopia [matching defects in the same hemifield of both eyes]
* Occipital lobe lesions- more congruous
* Retinal lesions- Defects are deep & hav sharp borders
* Diab r’pathy- Multifocal & mottled appear
* RD- Relative defects
* Retinoschisis- Absolute defect
* RP- Ring scotoma in mid-periphery [d/t more rod population in mid-periphery]→ Tunnel vision
* ARMD – Central scotoma
* CSR- central scotoma
* Retinochoroiditis- Arcuate defect
* Arterial occlusion- Absolute field defect
* Venous occlusion- Highly variable field loss.
CLOVERLEAF PATTERN-
Artifactual pattern
Threshold values are nml or near nml at & sometimes around the four primary points where the test begins, but are much reduced at other locations where the threshold is measured later in the test
This pattern occurs when the patient has responded more or less appropriately during the initial part of the test & then given up.
LASERS [j-04,j-03]
LIGHT AMPLIFICATION BY STIMULATED EMISSION OF RADIATION
Def-
Property to absorb light energy of one form & emit a new form of energy which is more useful.
LASER TISSUE INTERACTION-
2 variables-
1) LASER VARIABLE-
* Wavelength
* Spotsize
* Power
* Duration
2) TISSUE VARIABLE-
* Transparency
* Pigmentation
* Water content
-Only laser variables can be controlled.
-power is inversely proportional to spot size.Therefore if the spot size is decreased,the power must also be decreased to prevent a very intense burn
Laser tissue interaction-
Photocoagulation
Photovapourisation
Photodisruption
Photoablation
Photodynamic therapy
PHOTOCOAGULAION-
Photothermal phen
Pigment dependant
Xanthophyll-Both plexiform layers of retina
-Absorbs blue light max
Haemoglobin-BVs & H’ages
-Absorbs yellow light max
-Also blue & green
Melanin-RPE & choroids
-Absorbs entire visible spectrum
Pigment absorbs light energy→ Converted to heat energy → Temp elevation [10-20 deg C]→ protein denaturation→
Tissue atrophy→ seen after PRP
Thrombus formn
Collagen contraction
2) & 3) cause occlusion of vascular lumen→Focal photo of new Vs on retina
Undesirable effects of collagen contraction→
Membrane shrinkage→ Retinal traction
Beneficial effects of collagen contraction→
Pulls the peripheral iris out & away from the angle in peripheral iridoplasty
Lasers- Argon, krypton, dye , diode, freq doubled YAG
Use- PRP
-ALT
PHOTOVAPOURISATION-
Kronlein’s proc
Blepharoplasty
Iridotomies
Debulking of large conj tum
Undesirable effects-
Break in Bruch’s memb→ CNV
` Rupture of BV wall→ IO h’age
3. PHOTODISRUPTION-
* Independent of pigment
* Highly energized focal laser beam is delivered onto a tissue over a period of nanosec / picosec→ Optical breakdown → i.e Tissue is converted into an amalgam of neutrons, ions & free electrons → All of them collide with each other→ This amalgam is k/as ‘ plasma’→ collisions→ Electromagnetic & acoustic waves.
* These waves travel in all dir but rapidly dissipate resulting in a focal effect → Photodisruption
Eg- ND: YAG Capsulotomy
PHOTOABLATION-
-PTK
* Risk- Mutagenecity
-Alters structure of DNA & RNA
Read PDT & TTT from retina pg 83. folder.
LASER
|
WAVELENGTH
|
1. Ruby
|
694.3nm
|
2.Nd:YAG
|
1064nm
|
3. Double frequency Nd:YAG
|
532nm
|
4. Argon
|
488-514nm
|
5. Krypton
|
647nm
|
6. Diode
|
780-840nm
|
7. CO2
|
9000-11000nm
|
CLASSIFICATION-
SOLID STATE-
Ruby [694.3 nm]
Nd:YAG [1064nm]
Double frequency Nd: YAG [532nm]
GAS LASER-
Ion laser- Argon laser [488-514nm]
- Krypton laser [ 647nm]
b) CO2 [9000-1100nm]
METAL VAPOUR LASER-
Copper
Gold
EXCIMER LASER-
Argon fluoride-[ 193nm]
Krypton chloride-[222nm]
Krypton fluoride-[249nm]
DYE LASER-
RUBY LASER-
DIODE LASER-
TTT
ICG guided t/t of CNV
DME & PDR
Trabeculoplasty
Laser indirect O’scopy
Cyclophotoablation
Small size
Portable
No special electrical / cooling system
Little absorption of light in nuclear sclerosis
effect thru surface h’age
Better
Nd: YAG LASER-
Flash lamp
Continuous arc lamp
-There are 2 ways of pulsing Nd:YAG –
1) Q-switching
2) Mode-locking
Q-switching-
* A Shutter in front of one of the mirrors in the laser cavity blocks laser light emission until a large population inversion occurs→Shutter is opened quickly→ Stored energy bursts forward in the form of a brief pulse that lasts abt one-millionth of a second.
* Inexpensive
* Cannot produce pulses as short or powerful as mode-locking
* Most clinical Nd: YAG lasers today are Q-switched bcos mode-locked are more expensive & diff to maintain.
Mode-locking-
An optical element inside the cavity synchronises the mode.So all the light is emitted in brief pulses.
Binocular stereoscopic microscope
Two Helium-Neon [He-Ne] laser aiming & focusing beams aligned in such a way that they outline the cone of the invisible infra-red Nd:YAG beam .
APPLICATIONS-
1. Nd: YAG Capsulotomy-
IND- Posterior capsular opacification causing
-Decrease in V/A
-Diplopia
-Glare
-Invisible fundal glow
-Christmas tree
Complications-
Damage to IOL (pitting) d/t poor focusing
CME
Rheg RD
Increase IOP
Posterior IOL subluxation / dislocation
Chr endophthalmitis [ d/t release of sequestered org in vit]
Post-laser-
Topical Timolol 0.5 % e/d BD
Topical steroids for 7 days
2. Nd: YAG Iridotomy-
IND-
Prim angle closure glauc
Fellow eye in acute glauc
Narrow occludable angles
Sec angle closure with papillary block
TECH-
Apraclonidine 1% or Brimonidine 0.2%
Topical anaesthetic drop
Abraham’s lens
Site- Superior iris to avoid diplopia as it remains covered by lid
Beam shud be non-perpendicular
3 Bursts of 3-6 mJ
Gush of pigment debris
Post-laser- Apraclonidine 1% or Brimonidine 0.2 %
Topical steroid for 7 days
Ideal opening- 150- 200micron
COMPLICATIONS-
Bleeding
Iritis [d/t over t/t & inadequate postlaser steroid]
Cor burns
glare & diplopia
Other indications-
Nd: YAG vitreolysis
Cyclophotocoagulation
Iridolenticular synechiolysis
Persistent hyperplastic papillary membrane
Ant hyaloidotomy-For malignant glauc
Rupture of conj cyst
Radial iridotomy for rigid pupil
10 Laser sclerotomies
ADV-
High power density
Small coagulation
Cutting & lysing of small tiss
Low maintenance
Portable
DISADV-
High absorption by media
Potential for vascular rupture
Non-thermal action on adjacent tissue.
DYE LASER-
2 Types-
1) Thermal – Photo of post pole lesion
_ PDT
2) Pulsed- Laser sclerostomy
- Iridectomy
- Periorbital portwine stain
EXCIMER LASER-
USES-
PRK – For myopia
Phototherapeutic keratectomy for corneal scars
Sclerostomy
Trabeculectomy
PHACOABLATION-
Sculpting & ablative decomposition of cataract.
2 methods-
1. Ant surf of lens & deeper layers are blasted & the products removed by AC lavage
2. Fibreoptic probe introduced into AC &Cataract decomposed
LASER ASEPSIS-
Organism + Topical drop on cor containing antibody to this org tagged with Fluorescein→ Subjected to argon laser→ Fluorescein absorbs argon → converts it into heat energy→ Death of org
ELECTRORETINOGRAM
There exists a potential difference of 1mV bet the cornea & post pole of the eye k/as corneoretinal potential.This potential is modified by the action of light on the retina.The resultant waveform from modification in the corneoretinal potential in response to a brief flash of light is k/as Electroretinogram.
Thus the ERG is a composite of electrical activity from the photoreceptors, muller cells & RPE.
COMPONENTS OF ERG-
1) a-wave-
- Initial cornea negative wave
- Arises from photoreceptors [ rods & cones]
2) b-wave-
-Large cornea –positive wave
-Arises from muller cells
-Represents activity of bipolar cell layer.
- Oscillatory potential- Ripple of 3 or 4 small wavelets on the b-wave.
3) c-wave-
- prolonged positive wave with a lower amplitude
- Represents activity of RPE.
MEASUREMENT-
1. AMPLITUDE-
a) a-wave amplitude-
Measured from the baseline to the trough of a-wave
b) b-wave amplitude-
Measured from the trough of a-wave to the peak of b-wave
2. TIME SEQUENCES-
a) LATENCY-
Time interval bet the onset of stimulus & beginning of a-wave
Nml- 2msec
b) IMPLICIT TIME-
Time from the onset of light stim until the max a-wave or b-wave response
ERG RECORDING-
Application of electrodes-
1. Active / main electrode-
- Placed on the cornea, embedded in a contact lens
- Or Wick electrodes in the conj sac
- Or Skin electrodes of gold foil on eyelids
-This is the positive pole
2. Referance electrode
- Silver chloride electrode
-Placed on pt’s forehead.
- Serves as the negative pole.
3. Ground electrode
- Placed on the ear lobe.
RECORDING-
the contact lens electrode picks up the electrical potential that exists bet the neg post pole & positive cor foll light stim of retina
after arising at the contact lens,the signal is channeled thru consecutive devices for preamplification , amplification & final display.
PHOTOPIC VERSUS SCOTOPIC ERG-
PHOTOPIC ERG-
D/t cone response [ 5-8 million cones]
Under light –adapted condition
Lower amplitude & shorter implicit time
SCOTOPIC ERG-
D/t rod & cone response
6-8 million cones & 125 million rods
Recorded after 20 min of dark adaptation
Rod response can be isolated by stimulating the fully dark adapted eye with a flash of very dim light or blue light
Rod response gives reduced amplitude & longer implicit time
CLINICAL APPLICATIONS-
ERG can detect abnmlities upto bipolar cell layer.
It is nml in diseases inv ganglion cells & higher visual pathway such as optic atrophy
It measures diffuse responses of the retina, so isolated lesions cannot be detected like- localized macular h’age,macular holes,exudates,chorioretinitis & localized detachment
Retinitis pigmentosa-Marked reduction in amplitude
DR- Oscillatory potential is abolished. Disappearance of the wavelets suggests retinal ischaemia.Also seen in CRAO
RD-Immediate reduction in size of b-wave co-incidental with loss of vision.
ERG can be recorded even in the presence of dense opacities such as cor opacity, dense cataract & VH.
ABNORMAL ERG RESPONSE-
b-wave potential < 0.19 mV or > 0.54 mV→ abnml
1. Supernml response-
Potential above nml upper limit.
2. Subnml response- < 0.08mV
- Indicates that a large area of retina is not functioning.
- Seen in-
* Early RP
* Chloroquine & quinine toxicity
* RD
* Vit A def
* Hypothyroidism
* Mucopolysachharidoses
* anaemia
3. Extinguished response- Complete absence of response
* Adv RP
* Complete RD
* Adv siderosis bulbi
* Choroideremia
* Leber’s cong amaurosis
* Leutic chorioretinitis
4. Negative response-
-Large a-wave
* Arteriosclerosis
* Giant cell arteritis
* CRVO
* CRAO
PATHOLOGY
STAINS-
1] HAEMATOXYLIN & EOSIN-
- Nuclei [ DNA] – Stains blue
-Ribosome & Rough ER [RNA] – blue
- Cyto stains pink with eosin which is an acidic dye
2] PERIODIC ACID SCHIFF [PAS]-
- Stains glycogen,mucin,mucoprotein, glycoprotein & fungi
-Outlines tiss struct- BM, capsule &BVs
- Red
3] GRAM STAIN-
- + → blue / black
- - → Red
4] ZEIHL NELSON STAIN
- Blue background with red stain
5] ALIZANIAN RED>
- For Ca ++
-Red / brown
-Band KP
6] CONGO RED-
- For amyloid
Lattice dyst
Marilyn Monroe Always Gets Her Men in LA City
Macular dystrophy→ mucopolysacch→Alcian blue
Granular dys→Hyaline→Masson trichome
Lattice dys→Amyloid→ Congo red
GIANT CELLS
3 types-
1] Langerhan’s cells-
Peripheral horse-shoe shaped ring of nuclei
Eg-giant cell arteritis
2] FB cells-
Overlapped & centrally placed nuclei
3] TOUTON CELLS-
Ring of nuclei separate peripheral clear cyto from central eosinophilic cyto
-Eg – Juvenile xanthogranuloma
CONJUNCTIVAL NAEVI
MC site- bulbar conj
Types-
Junctional n- Between epith & substantia propria
Subepithelial- Below the epith
Compound n-Both epith & Subs propria
PTERYGIUM
DEF-Deg condition of the subconj tiss,which proliferates as a triangular fold to invade the cor, involving the BM & superficial stroma,the whole being covered by conj epith.
AETIO-
STAGES-
PROGRESSIVE STG-
-Thick,fleshy & vascular
-Gradually increases in size & encroaches onto the cor
-Stocker’s line-iron deposited as aline in front of the apex in core pith
2.ATROPHIC / STATIONARY-
-Thin,attenuated & with poor vascularity
PARTS-
-Apex / head
-neck
-body
-cap-semilunar infiltrative opaque spot in front of the apex
SYMPTOMS-
-Masss on nasal or temporal aspect
Read from basak-107
Diff from pinguecla-
Pt- usually nasal
Pi- nasal & temp
2.Pt- inv cor as well conj & destroys bowman’s memb
Pi-Confined to conj
H/P-Stromal elastosis / basophilic degeneration
- Normal conj shows eosinophilic stroma.
-Sun-->Conj collagen stains blue resembling elastic tiss→So elastotic /basophilic degn
-Also seen in-Actinic keratosis
-BCC
-SCC
-melanoma
OCULAR COHERENCE TOMOGRAPHY-
[j-07]
Non-invasive, non-contact imaging system
Prod micron-resolution retinal images in-vivo
Diode laser used
Analogous to B-scan ,instead of sound, it uses light
PRINCIPLE-
-A beam of near-infra-red light [830-850n] is directed into the tissue
-Using the principle of low-coherence interferometry time delay of reflected or backscattered light from the microstructures within the tiss is measured
-Optical –reflectivity is calculated by computerized image processing & images are displayed in false colour
-Bright colours [red to white]→High optical reflectivity [-50dB]
-Dark colours [blue to black]→low or no - “ -[-100dB]
-Axial resolution-10-15 µm
-Interpretation-
* The posterior red band corresponds to the RPE & choriocapillaris
* This layer terminates at the margin of the OD
* The anterior red band corresponds to the NFL.The NFL increases in thickness around the OD
* Bet these two red bands are ares of low reflectivity – neurosensory retina
* Two bands of intermediate reflectivity correspond to IPL & OPL within the neurosensory ret
-a light source is reflected onto a partially reflective mirror [optical beam splitter]
-One of the resulting beams is directed into the patient’s eye & reflected from IO structures
-This reflected beam consists of multiple echoes & provides information abt the distance & thickness of IO struc
- The second beam is reflected from a reference mirror at a known spatial location
-This beam travels back to the beam spilitter where it combines with the light reflected from the pt’s eye
-These two beams coincide & produce interference ,which is measured by a photodetector
Diag from notes
APPLICATIONS-
1] Macular holes-diag & staging
2] ERM-membrane thickness
-cystic changes
-focal vs global adherence to the ret surface
3]DME
4]CME
5] CSR
6]CNV
7] Postoper. Assessment of trabeculectomy site,AC angle & CB
DISADV-
1.High cost
2.Posterior subcap & cort cat impair performance
3.Pupillary dilatation is reqd for peripapillary measurement
ANTIOXIDANTS [j-07]
DEF- Substances whose presence in relatively low conc significantly inhibits the rate of oxidation of the targets
How do they work?
They serve as natural protectors in the body, mopping up free radicals & reactive oxygen species,which are potentially damaging.
They work in 4 ways-
Separate free radicals & reactive O2 species from the succeptible molecules in the body
Provide molecules which compete with O2
Rapidly repair the damage caused by free rad / O2 species
Lyse the free rad / reactive O2 species & remove them
Free radicals are chemical species having single unpaired electron in outer orbit.So they are very unstable.Antioxid give up electrons to free radicals thus thwarting their deletrious effects
Antioxidants-
Intracellular enzymes-
Catalase –present in peroxisomes
Superoxide dismutase-present in mito & cytosol
Glutathione peroxidase-protects cell injury by catalyzing free radical breakdown
Nutrients-
Vit A-anticarcinogenic
-Reduces susceptibility of LDL to oxidation
2. Vit E- “
3.Vit C-ascorbic acid
-scavenges oxygen radicals
-increases ferritin conc in lens epith→ferritin sequesters iron which catalyzes free rad
4.Cu
5.Se-helps glutathione peroxidase in catalyzing breakdown of peroxidase which produces ocular damage.
6.Fluorides
7. Nuts
8. Friuts
9veg, cereals, pulses
10.Zn-integral part of superoxide dismutase & catalase
-aids in capture of free rad release
-retards ARMD progression
IND-
ARMD
DR
ROP
Ischaemic ophthalmopathy
cor inflamn
POAG
Senile cataract
C/I-Hypersensitivity to any of its constituents
DOSE- one capsule/day
Suitable for diab as they do not contain any sugar
MIXCAROTIN-contains essential carotenoids-alpha carotene,beta carotene,cryptoxanthin,lutein & zeaxanthin.Derived from sea algae