

CORNEA
ANATOMY-notes
EMBRYOLOGY-
a)Epithelium-Formed from the surface ectoderm.
-Eyelids open at 5-6 mo of gestation,by which time the epith attains an adult appearance
b) Endothelium & DM-
Formed from mesenchymal cells derived from the neural crest,which are situated at the rim of the optic cup.
-40 days of gestn-endo contains 2 layers of flattened cells
-3rd mo endo becomes single layer of flattened cells that rest on their interrupted basal lamina,the future DM.
-6th mo DM is clearly demarcated.
c) Stroma & Bowman’s layer-
-from mesenchymal cells that insinuate between the surface ectoderm & developing lens
-Bowman’s layer starts forming by condensation of most superficial acellular stroma after 4 th mo. & is fully dev by birth
Corneal diameter:H-12, V-11
Anterior surface; Horizontal -11.7
Vertical -10.6
Posterior surface:Horizontal-11.7
:Vertical -11.7
Radius of curvature:
Ant:7.8
Post:6.5
Corneal thickness-central- 0.5- 0.6
-peripheral-1.2
Refractive power- 45 D
Refractive index -1.376
LAYERS-Epithelium/
-Bowman’s membrane
-Stroma
-Descemet’s membrane
-Endothelium
EPITHELIUM-Stratified squamous
-50-90μm
-Basal layer-columnar cells
-2-3 layers of wing or umbrella cells
-2 layers of flattened cells
BOWMAN’S LAYER –acellular mass of condensed collagen fibrils (superficial part of stroma)
-8-14µm
-does not regenerate
STROMA -0.5mm
-collagen fibrils & cells embedded in proteoglycans
-the lamellae are parallel to each other as well as to the cor plane.
-They have an oblique orientation in the ant 1/3rd & are at right angles to each other in the post 2/3rd
-This parallel arrangement allows easy intralamellar dissection in superficial k’tectomy & LK
DESCEMET’S MEMBRANE –Represents basement mem of the endo from
Which it is prod.
- 3µm –birth
-10-12µm-young adults
-40µm- senescence
-most resistant
-regenerates
-Stays in a state of tension but when torn it
Curls on itself.
-At the periphery it ends at the anterior limit
Of the trab meshwork as Schwalbe’s line
-periphery –Hassal henle bodies-ageing
-central – Guttate –Fuch’s dystrophy
ENDOTHELIUM –single layer of flat polygonal cells
-birth-6000cells/mm2
-adults-2400-3000cells/mm2
-<500 cells – cor. Decompensation
-highest mitochondria next to photoreceptors
-The endo cells are attached to the DM by hemidesmosomes & laterally to each other by tight junctional complexes.
-These linkages are calcium dependant &maintain the barrier function of the endo
-endo contains an active pump mech & is involved in active secretion & protein synthesis
BLOOD SUPPLY-avascular
ant. Ciliary Vs in subconj. Tissue invade 1mm of cor.periphery
NERVE SUPPLY- 5 n---ophthal.div----nasociliary n----→long
ciliary n-→enters the eyeball around the optic n along with short ciliary ns-→suprachoroidal space-→pierce the sclera a short distance near the limbus to leave the eyeball-→divide dichotomously -→pericorneal plexus of Ns-→1-2mm in the stroma they lose their myelin sheath-→stromal plexus-→subepithelial plexus-→penetrate pores in BM→extend betn epith. Cells→intraepithelial plexus
Nerve density highest in centre and decreases towards the periphery
PHYSIOLOGY
CORNEAL TRANSPARENCY [d-05]
Factors-
1.Homogenicity of ref. index of epith.& the transparent precorneal tear film
-2.Arrangement of stromal lamellae-
Maurice theory- collagen fibrils are arranged in a regular lattice so that scattered light is destroyed by the mutual interference.Cor will remain transparent so long as the fibrils are separated by less than a wavelength of light
Goldman theory-
Fibrils do not interfere with light transmission unless they are longer than one half a wavelength.
-3.Cor. avascularity
-Cir is avascular except for small loops which invade the periphery for 1mm.it facilitates nutrition,transport of sys antibiotics & drugs
-progressive vascularisatin is a harmful process as it interferes with transparency.
Factors affecting cor Vascularization-
A) Chemical theory-
- Role of Vasoinhibitory Factors (VIF)-Stromal glycosaminoglycan acts as a VIF.
-Role of Vasostimulatory factor ( VSF)-Release of VSF at the site of the lesion→diffuses thru the stroma to the limbus→stim new V growth from the limbal plexus.Hypoxia also stim VSF.
B) Mechanical theory-
Cogan postulated that BVs cannot invade nml cor bcos it is compact & that loosening of the compactness d/t edema was mandatory for NV.
But Langham said that edema alone is not responsible for NV.For eg,in Fuch’s Dystrophy & aphakic BKP it is rare for NV to occur even when there is edema
C) Combined Chemical & mechanical theory-
Maurice stated that both VSF & stromal loosening are necessary for NV
4 corneal hydration-
-Nml cor maintains a state of relative dehydration.
- The water content of nml cor is 80% which is kept in balance by factors which-
a) Draw water in the cornea-stromal swelling pressure
-IOP
Stromal swelling pressure is the keystone of cor biophysic It is a pressure ( 60mmHg) exerted by the GAG sot the stroma.The electrostatic repulsion of the anionic charges on the GAG molecule expands the tiss,sucking in the fld with equal but neg press called Imbibition pressure
IP = IOP – SP
= 17 -60
=-43 mm Hg.
b) Factors that prevent flow of water in the cor-
Epithelial & Endothelial barrier
c) Factors which draw water out of the cor-
Active pumping action of the endoth- Na + /K + ATPase pump
Disturbance of any of these factors→ Hydration > 80 % → cor thickness increases & Transparency decreases
BACTERIAL KERATITIS [J-01]-case
DEF-Loss of epithelium with inflamn in the surrounding cor
ETIO-Org-pseudomonas
-staph.aureus & albus
-pneumo
-org invading intact epith→gonococcus
Corynebacterium
listeria
-e.coli
Org. liberate toxins -→necrosis + pus formn -→ cor. Ulcer
CENTRAL COR.ULCER-viva
- Neurotrophic
- Atheromatous
- Exposure keratitis
- Keratomalacia
PERIPHERAL C.U-viva ( CASE) NOTES
*marginal keratitis
*mooren’s
*phlyctenular keratitis
* Terrien’s deg
*Rosacea keratitis
*Collagen vascular dis-
-RA
-SLE
-sjogren’s syn
-wegener’s granulomatosis
-PAN
-relapsing polychondritis
DEEP KERATITIS-
- IK
- Disciform keratitis
- Sclerosing keratitis
STERILE CU-
1.Post-infectious-metaherpetic-herpes simplex,bacterial,fungal
2.Traumatic-chem,thermal
3.postsurgical-homograft rejection
4.Lacrimal-keratoconj. Sicca
-sjogren’s syn
5Lids-ectropion/entropion
-trichiasis
-lagophthalmos
-exophthalmos
6.Neurological-neurotrophic keratitis [HZO,5n,DM]
-neuroparalytic exposure [7n palsy]
7.Immunological-collagen vas.dis
-mooren’s ulcer
8.Allergic –marginal ulcer
-vernal catarrh
9.Dermatologic –pemphigoid
-erhythema multiforme
10.Nutritional – keratomalacia
RISK FACTORS- VIVA
1- Trauma
2-Prolonged topical steroid
3-Dry eye
4 -entropion+trichiasis
5-Lagophthalmos
6 -Contact lens
7 -Dacryocystitis
8 -Poor local hygiene
9 -Bullous KP
PATHOLOGY-
STAGE OF PROGRESSION & INFILTRATION-
Infiltrn of the epith by PMN&lymphocytes from peripheral cir.-→ necrosis-→necrotic tiss cast off-→ saucer shaped defect.
STAGE OF REGRESSION-
Line of demarcation & wall of PMN leucocytes forms 2nd line of defence-→leucocytes macerate & dissolve the necrotic tiss which is shed off-→ surrounding infiltn & swelling disappear-→floor & edge become smooth & transparent-→vascularisation along the limbus to restore loss of subst
STAGE OF CICATRIZATION-
Regeneration of collagen & fibrous tiss formn-→ newly formed fib r irregularly arranged -→refract light irreg-→scar-→scar may not fill the gap exactly-→surface is flattened / indented-k/as FACET
C/F-SYMPTOMS-Acute onset
-Pain
-Redness
-Lacrimation
-Blepharospasm
-DOV
SIGNS-Lid edema
-Ciliary congestion
-Iritis
-Grayish white ,circumscribed cor infiltrate + edema of surrounding
Tiss. Margins overhanging. Floor- necrotic material
-Extent can be detected by fluor stain
-Hypopyon
-raised iop
CHARACTERISTICS OF CU-
- Staph aureus & stepto pneum-
- oval
- yellowish white
- dense& opaque stromal ulcer surr by relatively clear cor
- Pseudomonas-
- Greenish exud
- Irreg,deep ulcer with ground glass appear of surr stroma
- Rapid progression → perforation in48 hrs
- Enterobacteriaceae- ( Ecoli,proteus,kleb)
- Shallow ulcer
- Greyish white necrotic ulcer
- Ring shaped cor infiltrates
COMPLICATIONS-
Deep ulcer--→loss of tiss.-→ cor. Thinning-→ cor. Bulges under influence of nml iop-→ cicatrix becomes consolidated. Bulging may disappear / remain permanently as an ECTATIC CICATRIX
DM offers the greatest resistance to inflamn, but is unable to alone support the iop, so it herniates thru the ulcer as a transparent vesicle -→DESCEMETOCELE / KERATOCELE
PERFORATION & ITS EFFECTS-
Sudden exertion -→ raised iop-→ perforation-→ sudden escape of aqueous-→ fall in iop
Small perforation-→ iris gums down to the opening, adhesion organizes-→ (1) ANT.SYNECHIA-→ AC reformed & fresh aq. Secreted
CAUSES OF ANT SYNECHIA-
1.Perforated CU
2.Penetrating inj
3.Acute ACG
4.Iris bombe
Large perforation-→ iris prolapse-→ If total-→ whole cor sloughs with a narrow rim left-→ pupil becomes blocked with exud-→ false cor. Formed which consists of iris covered by exud which becomes organized -→forms a thin layer of connective tiss over which conj/cor e pith rapidly grow -→(2) PSEUDOCORNEA
Perforation-→Suspensory ligament ruptures -→ (3) Lens subluxation/dislocation/expulsion
Cicatrix becomes ectatic in which iris is incarcerated-→(4) ANT. STAPHYLOMA
If perforation occurs opp to the pupil-→ pupillary margin adheres to the edges-→ aperture fills with exud-→ AC reforms-→ lens long remains in contact with ulcer-→(5) ANT. CAPSULAR CATARACT
As the AC reforms, exud filling the opening is submitted to strain-→ ruptures -→(6) CORNEAL FISTULA
Perforation-→ sudden drop in iop-→ loss of support of BVs-→ rupture-→(6) IO h’age----Retinal Vs-→VH, Choroidal Vs-→subretinal/subchoroidal h’age
Org. causing ulcer gain access to the interior of eye-→(7) PURULENT IRIDOCYCLITIS /even PANOPHTHALMITIS
HYPOPYON COR ULCER-
Also k/as Ulcus Serpens
- Source of inf- Chr dacryocystitis
- Predisposing factors-
Virulence of infecting org & resistance of the tiss
- old debilitated pts
- Alcoholics
Mech of dev of hypopyon-
Iritis due to bacterial toxins
↓
Outpouring of leucocytes from the inflamed BVs
↓
Gravitate at the bottom of the AC-Hypopyon
This is not d/t actual invasion by the bact,so hypopyon is sterile
INVESTIGATIONS
1.Conj. sac & lid margins are swabbed & cultured
2.Corneal scrapping-collected from ulcer bed & margin with a kimura spatula / no. 15 blade.Topical anaesthesia [0.5% proparacaine / 4% lignocaine]-→Smears are made and culture media inoculated at pt’s bedside
strepto pneum recovered from the edge and moraxella from the base
CULTURE MEDIA- Bld. Agar
-Chocolate agar
-Thioglycolate broth
-Non-nutrient agar
-LJ med
STAINING PROCEDURES
GRAM STAIN- Fix smear in 95% methanol-→ Flood smear with crystal violet-→rinse with tap water-→ flood smear with Gram’s iodine-→ decolourize with acetone- alcohol→ rinse with tap water→flood with safranin /dilute carbol fuchsin→ rinse tap water & dry
GIEMSA STAIN→ Flood with giemsa’s soln for 45-60 min→ rinse in 95% ethanol
ZN STAIN→Flood fixed smear with hot strong carbol fuchsin & leave for 5min→ rinse with water→decolorize with H2SO4[20%]→ rinse with water→ flood with methylene blue counter stain for 2 min→ rinse with water→ dry
TREATMENT
1.Topical cycloplegic- mydriatic→ Relieves ciliary spasm
Prevents synechiae formn
[Atropine 1 % + Phenylepherine 10% ]
2.Hot fomentation → improves circulation & relieves pain
3.Analgesics
4.If raised iop-→ Tab. Acetazolamide 250mg qid
Timolol 0.5% e/d BD
5.Remove the source of inf- Discontinue contact lens
-DCT
-trichiasis – epilation
-FB removal
6.Fortified antibiotic drops
7.Debridement & Cauterization
Remove necrotic tiss with spatula & apply pure Carbolic acid 100% or trichloroacetic acid 20%
8.Corneal scars- superficial –Lamellar KP
-deep-Penetrating KP
9.Cor. scars with no visual potential-Cosmetic contact lens
-Tattooing with India ink or
Impregnation with gold [brown] or platinum [black]
10 FOR IMPENDING PERFORATION-
* Pressure patch bandage
* Lower the IOP-
-oral acetazolamide
-topical b-blocker
-paracentesis
* Glue
* Conj flap
* BCL
* Tectonic Graft
10.For perforated cor. Ulcer- Bandage soft CL
Tiss. Adhesive
-Therapeutic KP/ Conj. Flap
VIVA
- Keratitis- Corneal inflamn
- Superficial keratitis – anterior to DM
- Deep keratitis – in the stroma
- Epithelial defect – Loss of epithelium
- Abrasion / Erosion – Superficial epithelial defect without any inflamn
- Corneal ulcer – Epithelial defect with inflamn in the surrounding cor.
- Corneal abscess-Localized collection of pus in the cor with intact epith
- Scar – Opacity which follows inflamn
- Greatest cor. Sensitivity – central 5mm
- Infiltration –Cor. Inflamn with outpouring of leucocytes
CORNEAL OPACITY
– NEBULA – iris details visible [only Bowman’s
Memb inv]
-MACULA- Iris details not visible but iris & pupillary
Margin visible [ BM + ANT STROMA]
-LEUCOMA-Dense and white, totally obscuring iris
& pupil [Entire thickness of cor]
-Old & central leucoma shows a horizontal pigmented line
( Hudson Stahli line) at the palp aperture
*Adherant leucoma – Iris adherent to back of leucoma foll. Perforated CU
*Anterior staphyloma – Ectatic cicatrix with uveal incarceration
*Hypopyon – PMN leucocytes accumulate at the bottom of AC & become enmeshed in a fibrin network. Clinically it is pus in AC.
*Ulcus serpens – caused by pneumococcus
- Ulcer spreads over the cor. in a serpiginous fashion
-Ulcer spreads on the side of densest infiltration & on the other side undergoes cicatrisation
* Corneal abscess- Localised collection of pus in the cor subst.WITH INTACT EPITH
CORNEAL OPACITY-case
Look for-
- Grade
- Situation & extent in relation to the pupillary axis & limbus
- Any pigmentn
- Vascularisation-deep or superficial
-localized or circumferential
-site & extent
- Adherant leucoma
- Sensation
CORNEAL VASCULARISATION
` SUPERFICIAL DEEP
1..Can be traced over the limbus 1.End abruptly at limbus
Onto the conj.
2.Bright red 2.Greyish red
3.Well defined 3.Ill-defined
4.Branch dichotomously in an 4.Run parallel to each other in a
Radial dir.,branch at acute
Angle & course determined
By stromal lamellae.
Arborescent fashion
5.Raise the epith above them→ 5.Overlying cor. is smooth
Uneven surface
6.Derived from-conj 6.Derived from ant.ciliary Vs
CORNEAL VASCULARIZATION-
SUPERFICIAL- TPR
- Trachoma
- phlyctenular KC
- superficial CU
- Rosacea keratitis
DEEP-
- Interstitial keratitis
- Deep CU
- Disciform keratitis
- Sclerosing keratitis
- Chem burns
RX-
- Topical steroids-Vasoconstrictive action
- Radiation therapy-more useful in superf v
- Sx peritomy
DECREASED CORNEAL SENSATION
1.Lesions of 5n-oph div –surgery –ref. surg
-cor. graft
-Acoustic neuroma
-Trauma
2.Inf- HSV, HZV, LEPROSY
3.Contact lens
4.DM
5.Topical – anaesthetics
-β blockers
-NSAIDS
-Atropine
6.Neuroparalytic keratitis
7.Laser
8.Myaesthenia gravis
ORGANISMS PENETRATING INTACT EPITH
- corynebacterium diphtherium
- gonococci
- meningococci
- H.aeg
- Listeria
- Shigella
CORNEAL ULCER WITH HYPOPYON
- Pneumococcal
- Pseudomonas pyocyanea
- Gonococcus
- Staph
- Strepto
- moraxella
- fungal-aspergillus,Fusarium,Candida
Any CU may be asstd with a hypopyon but it is not analogous to hypopyon CU ( ulcus serpens)
NON-HEALING CORNEAL ULCER
CAUSES-
LOCAL-
- Raised IOP
- Concretions
- Misdirected cilia
- Impacted FB
- Dacryocystitis
- Lagophthalmos
SYSTEMIC-
- DM
- Severe anaemia
- Malnutrition
- Chr debilitation
- Sys steroids
Rx-
- Mechanical debridement or scraping the floor of the ulcer to hasten healing
- Cauterisation with Carbolic acid 100% or trichloroacetic acid 20 %
- SBCL
ANTIBIOTICS [D-03]
FORTIFIED ANTIBIOTIC DROPS-SPOT
1.F. CEPHAZOLIN 5% [ 50mg/ml]
500mg powder + add sterile water → make 10ml soln
2. F. VANCOMYCIN 0.3%
500mg powder + add sw -→ 10ml soln
3. F. TOBRAMYCIN 1.3% [13.6mg/ml]
Inj. 2ml tobra [40mg/ml] + 5ml commercial bottle of 0.3% tobramycin e/d
4. F. GENTAMYCIN [14mg/ml ]
Inj. Genta 40mg/ml + genta e/d
5. F. AMIKACIN [50mg/ml]
Inj. Amik. 500mg + 10ml sw
6. F. KETACONAZOLE [40mg/ml]
Tab.ketaconazole 200mg -2 Tab + 10ml sw
1} CEPHALOSPORINS
1st GENERATION – gm + [more]
- gm- [less]
* Cephalexin
* Cephadroxyl
*Cephazolin
2nd GENERATION- GM + [more]
-GM- [Neisseria, H.inf ]
*Cefuroxime – soft tiss inf
*Cefaclor
3rd GENERATION-GM – [more]
*Cefotaxime
*Ceftriaxone [monocef]
*Ceftazidime[fortum] --- pseudomonas – retinotoxic
*Cefixime,
*Cefpodoxime[metoxime]
4th GENERATION-
*Cefipime
*Cefpirome
For parental use. Serios hospital acqd inf
All cephalosporins are NEPHROTOXIC.
2} FLUOROQUINOLONES [D-02]
1ST GENERATION – Ciprofloxacin-arrhythmogenic
-2ND GENERATION –Ofloxacin- “
- Sparfloxacin- “
3RD GENERATION – Levofloxacin
4TH GENERATION – Gatifloxacin
- Moxifloxacin
Mech of action - bactericidal
Inhibit DNA isomerase → uncontrolled synthesis of mRNA & protein
Moxifloxacin –
Inhibit DNA gyrase & inhibit topoisomerase → inhibit DNA supercoiling → DNA replication
Organisms covered→ gm – e coli
Salmonella
Shigella
Proteus
Kleb
Gm + → staph & strepto
Pseudomonas
Atypical pneum – legionella
-listeria
-chlamydia
All F are not effective against anaerobes except gati & moxi
Side effect – arrhythmogenic
-cartilage toxicity
- subcapsular cataract
MOXIFLOXACIN –
- Topical 0.5% tds for 7 days
- Preservative free
- Safe in children & newborn
3} AMINOGLYCOSIDES
MOA – Attach to 50s or 30s ribosomal subunit → inhibit protein synthesis
- Bactericidal
- Mostly cover GM –ve
- Act at nuclear level [ while Pn act at cell wall level ]
DRUGS –1] Streptomycin
2] amikacin
3] Gentamicin 0.3 – 2% e/d-macular infarction
4] Tobramycin 1-1.4% e/d
5] Netilmycin
6] Soframycin [framycetin ] 0.5% e/d . NOT ORAL
7] Neomycin 0.3 -0.5% NOT ORAL
SIDE-EFFECTS – Nephrotoxic
-Ototoxic
-NM weakness
- Retinotoxic
-Macular infarction
4} MACROLIDES
MOA – Bacteriostatic
-Bind to 50s subunit of ribosome → Inhibit Bacterial cell wall synthesis
Org –GM +ve
-chlamydia
Toxoplasma
DRUGS –Emycin
-azithromycin
-clindamycin
-lincomycin
\
FUNGAL CORNEAL ULCER-case
[ D-01,D-02, J-02, D-03,D-05]
3 Types of fungi-
1. FILAMENTOUS –Fusarium solani
-aspergillus
-curvularia
2.YEAST- Candida albicans
-c. parapsilosis
-c.tropicalis
3.DIMORPHIC FUNGI –histoplasma
-Coccidiodomycosis
AETIOLOGY -1.Trauma with veg matter
-2.Protracted epith ulceratn
-3.Penetrating KP
-4.Therapeutic soft CL wear
SYMPTOMS –FB sensation
-Photophobia
SIGNS- Grayish stromal infiltrate
-Dull dry surface with feathery borders
-surrounded by yellow line of demarcation
-From the line of demarcation dark radiating lines spread into surr.
Tiss.
-Line of dem. Deepens into a gutter →infiltrn area sloughed off→ extensive ulcer .
-Massive hypopyon
-Perforation rare
-Satellite lesion
-Immune ring of wessely
-Cor. vascularization INCONSPIQUOUSLYabsent
T/T- [J-07]
INVEST-1.Corneal scraping-Scrape from the margin of the ulcer to include
The feathery edges
2.Culture media –1) Blood agar [aerobic]
-2) Chocolate agar
3) Sabouraud’s dextrose agar
4) Thioglycolate broth [anaerobic]
5) Brain Heart infusion broth [aerobic]
3.Stain-KOH stain [most basic test]
-Gram’s stain
-Giemsa’s stain
-Gomori’s methaneamine stain
-PAS
Special stains- -Acridine orange-stains RNA- orange red & DNA-yellow green
-Calcoflour white-fungi & acanthamoeba
4.Confocal microscopy & electron microscopy-direct in-vivo
visualization of fungal elements in the cor stroma
5. Molecular method-PCR & nucleic acid probe testing
6. Corneal biopsy-indicated in deep stromal infiltrate
TREATMENT-
1.Filamentous fungi-Natamycin 5% e/d 1 hrly
-Amphotericin –B 0.15% e/d
Candida-Imidazole 1% e/d
- Flucytosine 1 % e/d
2. Cycloplegics
3..Systemic –Tab. Ketoconazole 200 – 800mg /day for 7days
OR –Tab.Fluconazole 200mg/day for 3-4 weeks
4.SURGICAL T/T- –Therapeutic PK [D-05]
Ind-unresponsive cases
-Descemetocele
-perforation
-sev pain
* size of the graft is decided on the basis of size of ulcer & shud include the infected edges
OTHER-
- Adhesive & BCL
- Tarsorrhaphy
- Conj hooding
ANTIFUNGALS
3 groups – 1. POLYENES –Amphotericin –B ( liposomal amphotericin B)
-Nystatin
-Natamycin
-2 AZOLES.A} IMIDAZOLES –Ketoconazole
-Miconazole
-Econazole
-clotrimazole
-voriconazole
B} TRIAZOLES-
-Fluconazole
-Itraconazole
-3.PYRIMIDINES-5- Fluorocytocine
4. Caspofungine
5.anidulafungine
AMPHOTERICIN-B- [SN]
- Polyene
- Fungistatic & Fungicidal
- MOA- Binds to ergosterol in the cell membrane→ Impairs memb barrier function, loss of cell constituents & cell death.
- DOC- for yeasts
- Poor corneal penetration
- DOSE-
-Topical- 0.15 % E/D and 2.5 % E/O
-subconj- 0.37 mg
-Intravitreal- 5µg /0.1ml
-IV-available in 50 mg vial
Eye drops are not available commercially.They are prepared from inj AMB [50mg dry powder].The powder is divided into 6 equal parts of 8 mg each.Each part is then reconstituted with 5ml DW & placed in an amber coloured bottle.Hav to be used in 48 hrs. .
-Suspended in 10ml water & then diluted to 500ml with 5 %
Dextrose.Initially 1mg test dose is injected IV over 20 min. If no serious reaction follows, 0.3 mg/kg is infused 4-8 hrs.
Total dose upto 4gm can be given over 2-3 months.
- USES-
- Aspergilloses
- Blastomycosis
- Candidiasis
- Cryptococcosis
- Coccidiodomycosis
- Histoplasmosis
- S/E-
- Hypokalemia
- Anemia
- Renal tubular acidosis [ most serious]
- Thrombophlebitis
NYSTATIN-
- Fungistatic & fungicidal
- MOA- same as AMB
- DOSE- 5 % E/D & 3.5 % E/O
- USES- Candida
-aspergillus
NATAMYCIN-
- Fungicidal
- DOSE- 5% suspension
* USES-
1. Candida
2. Cephalosporium
3. Aspergillosis
4. Fusarium
5. Penicillium
- S/E- Epithelial ulceration
KETOCONAZOLE-
- Fungicidal
- DOSE- 1-5 % -topical
-oral- 200-800mg daily for 7 days
-Intravit- 0.5mg
* USES-
1. Candida
2. Fungal endophthalmitis
3.Fungal canaliculitis
4. Fungal blepharitis
5.Fungal conjunctivitis
6. Fungal cor ulcer.
- S/E-
- Nausea & vomiting
- Paraesthesia
- Gynaecomastia
- Loss of hair & libido
- C/I-
Pregnancy & lactation
ITRACONAZOLE- [SN]
- Synthetic diaxolone triazole compound
- MOA- Interferes in the formn of ergosterol→ disturbed cell memb functn
- DOSE- Topical- 1 % sol
-oral-100-400mg /day
* S/E- Nausea ,headache, abd pain
FLUCONAZOLE-
- Fungicidal
- MOA- Alters cell memb function→ leakage of essential elements.
- DOSE-Topical- 0.2 -2%
-oral- 200mg daily for 3-4 wks
-intravit- 0.1mg
* USE- Aspergillus , candida
-Cryptococcus retinitis
* S/E
1. Nausea
2. Abd pain
3. Headache
4. rash
MICONAZOLE-
- Fungicidal
- DOSE- topical- 1 % E/D
-2% E/O
* USE-
1. Candida
2. Aspergillus
3. Gm +ve bact
5 – FLUOROCYTOSINE-
* Fungicidal
* DOSE- topical -1 %
-oral- 200mg/day
* USE- Candida
-Cryptococcosis
-Aspergillus
HERPES ZOSTER OPHTHALMICUS [J-04,j-05]
Agent-Varicella zoster virus
Chickenpox in childhood/youth → virus lies dormant in gasserian ganglion →fall in immunity→virus travels down oph.br. of 5th n→eye
→skin
Herpes zoster ophthalmicus-
HZ affecting oph.br of 5th n irrespective of ocular inv.
HUTCHINSON’S SIGN-
When tip of the nose is affected, the eye will also be involved,since both are supplied by the Nasociliary N.
Age – 5-6 decade
Clinical phases- 1. Acute –Dev within 3 weeks
2. Chronic- persist upto 10 years
3. Recurrent –Re-appear after 10 years
ACUTE PHASE
1]An influenza like illness- fever, malaise,headache
2]Pre-herpetic neuralgia- Along oph. Div of 5th n
-Itching,tingling,or burning to a severe deep
Boring or lancing pain
3]Skin rash- Macules→ Papules→Vessicles→Pustules→ crusts→Scar
-Dermatomal distribtn. & respects the midline
4] KERATITIS-Acute epithelial
-Nummular
-Disciform
1] ACUTE EPITHELIAL- Small, fine, dendritic / stellate lesion→ Tapered ends & lack end- bulbs
2] NUMMULAR- Multiple, granular sub-epith. Deposits Surrounded by a halo of stromal haze.
3] DISCIFORM – always preceded by num. ker.
-axial
COMPLICATIONS- 1. Conjunctivitis
-2.Episcleritis
-3.Scleritis
-4.Iritis
-5.Ant.uveitis→ Sectoral iris atrophy
-6.Cranial nerve palsies-3, 4, 6, 7
-7.Optic neuritis
-8.Acute retinal necrosis [after 5 days- 3 mo of skin inf]
CHRONIC PHASE-
- Nummular keratitis
- Disciform keratitis
- Neurotrophic keratitis
- Mucus plaque keratitis
Other ocular complications- Scarring→ptosis
→ trichiasis
→ madorosis
→ notching of lid margin
-scleritis
-Mucus secreting conjunctivitis
-Post-herpetic neuralgia
RELAPSING PHASE-
1.Episcleritis
2.Scleritis
3. Iritis
4.Glaucoma
5.Keratitis
TREATMENT
- Tab.Acyclovir 800mg 5 times/day for 10 days
→reduces period of viral shedding
→Increases healing time by 50 %
→Reduces incidence of new lesions
→Reduces severity of acute pain
→Administer within 4 days of rash
2.Oral analgesics
3.Topical steroid – antibiotic cream –Hydrocortisone-1% + Fusidic acid 2% or oxytetracycline 3% until crusts have separated
4.For scleritis, sclerokeratitis or iritis→ Dexamethasone 0.1% e/d 4 hrly
Acyclovir e/o 5 times aday
5.for proptosis + 3rd n palsy + optic neuritis→ Tab. Pred. 60 mg / day
6. Dry eyes → Artificial tears
7. Neurotrophic ulcer → lateral tarsorraphy
HERPES SIMPLEX KERATITIS
HSV - DNA virus
HSV 1- Nose, lips & eyes
HSV2-Genitals
Primary infn-early childhood
-maternal antibodies-protection upto 1st 6mo of life
Recurrent dis - prim inf →virus travels up sensory n→ ganglion –HSV 1 –Trigeminal ganglion ,HSV 2 –Spinal ganglion → Latent phase → reversal of latency → Reactivates & replicates → along sensory n → target tissue
HSV→ 1.Primary ocular infection
2.Epith keratitis
3.Disciform keratitis
4.Stromal keratitis
1] Primary ocular inf → 6mo-5yrs
→Blepharoconjunctivitis
→Skin lesions –lids & periorbital areas
→Follicular conjunctivitis –acute & unilateral
→ Secondary canalicular obstrn
→ treat – acyclovir e/o 5 /day for 3 wks
2] Epithelial keratitis→
Opaque epith. Cells [punctuate/stellate pattern]→ central desquamation→ Dendritic ulcer [linear branching with terminal end bulbs].Bed of ulcer → fluorescein, virus laden margin takes up rose Bengal
Decreased cor sensation
→Dendritic ulcer → centrifugal enlargement → Geographic ulcer [larger epith defect]→ healing→ persistent linear branching shapes → Pseudodendrites → resolve with no scar
Treatment→1. Acyclovir e/o 3% 5 times/day
2.Ganciclovir 0.15 % gel 5 times/day
3. Trifluorothymidine 1% e/d 2 hrly /day
4.Debridement –For dendritic ulcer & not geog. Ulcer
-Removes virus laden cells & protects adjacent
Healthy cells
5.Prophylactic syst t/t
→ 2/ more attacks of epith keratitis
→ Oral acyclovir 400mg Bd for 1 year
3] DISCIFORM KERATITIS
*Immunological arthus reaction
*Central zone of epith. Edema overlying stromal thickening + KPs +folds in DM
* surrounding Wessely ring of stromal ppts
* Mild ant. Uveitis
* raised IOP
* T/T- Topical steroid
-Topical antiviral
4] STROMAL NECROTIC KERATITIS
*Cheesy necrotic stroma
*Ant uveitis + KPs underlying area of active stromal infiltrn
* Scarring
* Vascularization
*Lipid keratopathy
*Perforation
* T/T –top. Steroid
-Top. Antiviral
-Cycloplegics
ANTIVIRALS
- PYRIMIDINE DERIVATIVES-
- Idoxuridine-0.1 % E/D 2 hrly
- Trifluorothymidine 1 % 5 /d
- PURINE DERIVATIVES-
- Acyclovir
- Ganciclovir
- Others-
- Foscarnet
- Ziduvudine
IDOXURIDINE-
- Pyrimidine derive
- MOA- Inhibits DNA synthesis
- Prevents replication of herpes virus
- USES-Prim & recurrent herpes simplex keratitis
- DOSE- E/D 0.1 % every 2 hrly
-E/O 0.5 % HS for 2wks
* S/E-
1. Superficial punctate keratitis
2. Follicular c’vitis
3. Punctal occlusion
TRIFLUOROTHYMIDINE-
- Pyrimidine der
- MOA- Inhibits DNA replication
- DOSE- 1 % E/D 5 /day for 2 wks
- USES- DOC in HSV keratitis
- S/E-
- Burning / stinging
- Conj hyperemia & edema
- Keratitis sicca
- Delayed cor wound healing
- Rise in IOP
ACYCLOVIR-
- Purine derive
- MOA- Virustatic
-Inhibits DNA synthesis & viral replication
* DOSE- E/O 3 % 5 /day
-Oral- HSV- 400mg 5 /day for 7 days
- HZO-800mg 5 / day for 10 days
-IV – 500mg /kg over 1 hr ,repeated 8hrly for 10 days
* USES-
1. Herpes simplex keratitis
2. HZO
3.Epstein Barr virus
4 .CMV
5. Acute retinal necrosis
- S/E-
- Tingling & burning sensation
- Depostion of crystallized drug in the kidney
GANCICLOVIR-
- Purine der
- MOA-Inhibits DNA SYNTHESIS
- DOSE- 0.15% gel 5 /day
- oral – 1gm TDS with meals
-IV- 10 mg /kg BD for 14 days f/b 5mg/kg 12hrly
-Intravitreal- 200-2000µg /0.1ml
- Implant- releases 1 µg / hour
* USES- CMV retinitis
-HSV keratitis
-PORN
* S/E- Nephrotoxic
FOSCARNET-
- MOA- Inhibits replication of human herpes & retrovirus
- DOSE- IV 90 mg/kg BD →90 mg/kg OD for 2-3 wks
- USES- Only for sev CMV retinitis acyclovir resistance in PORN
- S/E- Nephrotoxic
-Neurotoxic
ACANTHAMOEBA KERATITIS
[D-02, J-02, D-04]
Ubiquitous free living protozoa
Found in air, soil,brackish water
Acanthamoeba →Cystic form
→Trophozoite
Cystic form →.under appro. Environmental Conditions,→Trophozoite→ enzymes→Tissue penetration & destruction of epith.-->stroma→ AC
PREDISPOSING FACTORS-
- Soft CL wearers using contaminated lens soln
- Minor cor. abrasion
- Swimming / bathing in contaminated water
May coexist with herpetic keratitis
SYMPTOMS- Blurred vision
-Sev. Pain
SIGNS-* limbitis
*Patchy stromal & perineural infiltrates [i.e along the cor. Ns]
*Overlying epith → intact
→Punctate keratitis / pseudodendrites
*Gradual enlargement of infiltrates→coalescence→central/paracentral Ring abscess
*satellite lesion
*slowly prog.stromal opacification→ descemetocele
INVEST
*Staining & microbiological exam of –cor scraping [epith]
-Biopsy [stromal inv]
-contact lens case
With calcoflour white stain –chemifluorescent dye with affinity for amoebic cyst wall
- Cultures –Non-Nutrient agar seeded with e.coli or buffered charcoal yeast extract [BCYE]
- *PCR-detection of acanthamoeba DNA from epith scrapings / tears
T/T-
1. Topical amoebicides –
A] Propamidine isothionate 0.1% + polyhexamethylene biguanide 0.02% [PHMB]
B] Neomycin + miconazole
C] Chlorhexidine
2.Topical steroid
3.Therapeutic PK→-Avoid in inflamed eye
-do wen inf has resolved to restore cor. clarity
MOOREN’S ULCER [j-02]
Also k/as Rodent ulcer or chronic serpiginous ulcer
* degenerative & superficial
*autoimmune response to stromal antigen
*spread of ulcer- →
underlying cause – ischaemia→ autoimmune lysis of epith → collagenolytic enzymes → erosion→ grey infiltrates 2-3mm from limbus→ breakdown → small ulcers → spread & coalesce → ulcer undermines the epith. & superficial stromal lamellae at the advancing border→ whitish overhanging edge with base vascularised→ circumferential & central spread→. Healing → Thinning→ vascularisation → Scarring
*Secondary cataract
*perforation rare
* sclera uninvolved
CLASSIFICATION-1
1] UNILATERAL ULCERATION-Elderly
-female
-Extremely painful
-prog. Ulceration
-Obliteration of superficial juxtalimbal vascular plexus
2]BILATERAL AGGRESSIVE ULCERATION[ MALIGNANT FORM]
-young
-males
-C/F *less painful
*prog circumferential ulceration with late centripetal spread
*FA- Neovascular n with leakage into base
3] BILATERAL INDOLENT ULCERATION
-Middle aged
-Malnourished
-Prog peripheral ulcer
-Min inflame
-
T/T
1] Topical steroid
2] Topical cycloplegic
3] Pulsed steroid
4] 4mm excision of adjacent conjunctiva→ eliminates source of collagenase,proteoglycanase
5] Perforation→ Debridement →Cyanoacrylate + BCL
6] Lamellar KP
7] IV. Methotrexate 7.5 -15mg/ wk
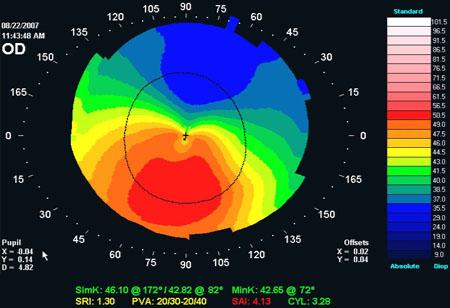
KERATOCONUS [D-02]-spot-cor topo
DEF→Progressive disorder in which cor has an irreg conical shape
EPIDEMIOLOGY→
*onset at puberty
*Bilateral
*AD transmission with incomplete penetrance
ASSOCIATION→
Systemic-
* Downs
* turners
* Ehler danlos
* Marfan’s
* Atopy
* Osteogenesis imperfecta
* Mitral valve prolapse
OCULAR-
*Vernal kc
*Blue sclera
*Ectopia lentis
*Leber’s congenital amaurosis
*RP
Predisposing factors-
*Rigid CL wear
*Constant eye rubbing
MORPHOLOGICAL CLASSIFICATION→
1] Nipple cones
* small [5mm]
* steep curvature
* apex- central/paracentral
* displaced inferonasally
2]Oval cones-
* larger [5-6mm]
* ellipsoid
* displaced inferotemporally
3] Globus cones
* largest [>6mm]
SYMPTOMS→
* Unilateral impaired vision [d/t myopia & astigmatism]
* Frequent change in spec correction
* CL intolerance
SIGNS
1] Early signs-
1) Direct o’scopy- “OIL DROPLET REFLEX”
2) Retinoscopy-“SCISSOR REFLEX”
3) Slit lamp –VOGT’S STRIAE –fine vertical, deep stromal striae which disappear on pressure
4) Prominent corneal ns
5) Keratometry shows irreg astigmatism.Mires cannot be superimposed
6) Corneal topography- most sensitive for very early keratoconus
2] Late signs-
* MUNSON’S SIGN- Bulging of lower lid in down gaze
* FLEISCHER RING-Epith. Iron deposit around base of cone
* stromal scarring
3] Acute hydrops
* Rupture in DM→ acute influx of aqueous into cor
* Heals within 6-10wks
* Keratoplasty should be deferred till edema has resolved
PATHOLOGY- [D-01]
- Central stromal thinning
- Irreg epith
- Breaks in Bowmann’s layer with fibrosis filling the breaks that extend beyond the epith
- Hydrops- breaks in DM with inward curling
- Electron micro-Reduced thickness of cor with fewer lamellae & space bet the coll fibrils is increased
INV-
1] Computerised videokeratography-Detects early keratoconus
-follow progression
-to fit CL
2] placido based topography- shows inf steepening
3]Pachmetry- thinning of paracentral zone
T/T-
1] SPECTACLES-for regular/mild irreg astig.
2] CONTACT LENS-
→RIGID CL with 3-point touch tech-
A light central touch[2-3mm at the apex] & another touch at the periphery [3-9o’clock pos]
→SOPER’S TECH-Lenses with 2 posterior curves, one to fit central cone & other to fit normal cor surrounding the cone
→PIGGYBACK LENSES
3] EPIKERATOPLASTY
* Pts intolerant to CL
* Without significant central cor. scarring
4] KERATOPLASTY
*Penetrating/deep
*Advanced dis with cor. Scarring
5] Deep anterior lamellar KP
6] Intrastromal rings-
-Circular rings of PMMA are placed in the mid-peripheral cor stroma in a lamellar channel
7] Corneal collagen cross linking with riboflavin
- Corneal epith is removed
- Riboflavin drops applied
-Eye exposed to UV-A
-UV-A + riboflavin
-Reactive oxygen molecules
-Formation of chemical bonds bet & within the collagen fib, making them stiffer
VIVA-Breaks in DM-
- keratoconus
- cong glaucoma
- trauma in forceps delivery
WITH THE RULE ASTIGMATISM- 
AGAINST THE RULE ASTIGMATISM
PELLUCID’S MARGINAL DEGENERATION-SPOT-cor topo
- 3rd-4th decade
- Bilateral
- Crescent shaped inferior thinning of cor extending from 4-8 o’clock
- Seperated from limbus by clear normal cor
- Central cor protrudes over the area of thinning→ flattening the vertical meridian→ irreg against the rule astig
- Fleisher’ ring &vogt’s striae do NOT occur
- T/T→
*spec –fail
*Gas-permeable CL- best option
*Surgery-Wedge shaped resection of diseased tiss,penetrating KP,Crescentic lamellar KP,ThermoKPs

AMNIOTIC MEMBRANE
TRANSPLANT [J-04,J-05,J-07]
Innermost lining of fetus
- Thick Basement membrane + Avascular stroma
- PROPERTIES OF AM-
*Downregulates inflamn
*Upregulates healing
*Ideal substrate for growth of epith cells
*Facilitates epith cell migration
*Reinforces adhesion bet basal epith cells
*promotes epith cell differentiation
*Prevents apoptosis
*No adverse rea of rejection
STORAGE-
→obtained after caeserian sec delivery
→Screened for HIV, hepatitis, syphillis
→Placenta cleaned of blood & washed with sterile buffered saline soln containing-Pn G- 50mg/ml [GM+]
-streptomycin-50mg/ml [gm-ve]
-neomycin 100mg/ml [gm+]
-amphotericin-B 2.5mg/ml
→Amnion is separated from chorion by blunt dissection with gloved hand
→Flattened on a nitrocellulose paper with epith BM facing away from the paper
→Paper with adherent AM is cut into 3×4cm sheets & stored at -80 deg c in a sterile vial containing Dulbecco –modified Eagle med & glycerol
INDICATIONS-
1. Persistent epith defect
2. Sterile ulceratn
3. Descemetocele
4. Cor. perforation
5. Scleral perforation
6. Adjunct to limbal stem cell
7. Chem./thermal burns
8. After -excision of conj intraepith neoplasia
-symblepharon
-conjunctivochalasis
-pterygium
TECHNIQUE
3 ways- inlay
-onlay
-filling
INLAY-AM larger than epith defect is taken & sutured with epith
Side facing up,thus creating a surface on which new epith
Cells can grow.
ONLAY-Orientation is not important
-AM is placed over the entire cor, limbus &perilimbal
area like a biological CL
FILLING-For deep stromal ulcer
-Multiple layers of AM are used to fill the ulcer cavity
-After am transplant, a hydrophyllic bandage CL
Is applied
COMPLICATIONS-
- PO irritation & pain
- AM dehiscence
- wound leak
LIMBAL STEM CELL DEFICIENCY & TRANSPLANTATION [D-02,J-04]
STEM CELLS
- Located in limbal palisades of vogt
- Cor. epith is subjected to constant renewal & regeneration
- Cells in upper cor. are desquamated → LSC divide into daughter cells→ transform into Transient amplifying cells→Terminally differentiated cells→Healthy cor. epith cells.
- Destruction of LSC→Healthy cor epith cells will not fill the surf. Defects→Persistent epith defect→ Invites vascularization & conjunctivalization[ growth of cells of conj. Phenotype on cor surf]
- Characteristics- long life span
-low mitotic activity
-least differentiated
LSC DEFICIENCY
AETIOLOGY-
A] Primary –Aniridia
-Cong. Erythrokeratoderma
-Keratitis asstd with multiple endocrine def
-Chr. Limbitis
B]Secondary- Chem/thermal burns
-Stevens Johnson’s syn
-Ocular pemphigoid
-limbal surgery
-CL wear
-Microbial inf
SYMPTOMS-
*DOV
*Photophobia
*Tearing
*Blepharospasm
*Recurrent pain
SIGNS
*Irreg dull cor. epith reflex
*Thick fibrovascular pannus
*Scarring
*Calcification
*Persistent epi def
*Cor melting & perforation
INV-Conjunctival impression cytology- diag confirmed by prescence of goblet cells
-Cellulose acetate paper strip is applied near the limbus on bulbar conj inferonasally & inferotemporally.
-A glass rod is pressed on the paper for 3-5 seconds
-Strip is removed with a peeling motion
-Strip stained with PAS & haematoxylin
-Slide examined under light microscope
-Goblet cells are identified by intracellular mucin which is deeply PAS positive.
LIMBAL TRANSPLANTATION
Donor-unilateral- fellow eye [limbal autograft]
-bilateral- living related donor or cadaver [limbal allograft]
PROCEDURE-
Preparatory 360 degree peritomy & superficial keratectomy→100 micron deep bed , corresponding to the harvested donor tiss is prepared→semi-annular ,150micron thick donor graft is harvested→graft sutured onto recipient eye with interrupted 10-0nylon
COMPLICATION –Graft rejection
VIVA
HYPOPYON-
- Inf cor ulcer
- Endophthalmitis
- Retained lens matter
- Retained IOFB
- Iridocyclitis
- IO tumour necrosis
CORNEAL EDEMA-
Q-Causes & mgt [D-05]
CONGENITAL-
- Cong glaucoma [G’tomy,trabeculotomy,trabeculectomy]
- CHED [PKP]
- Post polymorphous dystrophy[T/T not reqd]
- Birth trauma
ACQUIRED-
- PO edema
- Bullous KP [Med-Anti-glauc,hypertonic agents,BCL
Surg-conj flap,AMT,BM cauterization,Ant
Stromal micropuncture,annular keratotomyPTK,PK]
- Fuch’s endo dystrophy[hypertonic ag,BCL,PK]
- CL overwear [disuse,HA]
- Trauma
- Ac angle closure glaucoma [antiglauc]
- Acute hydrops ( Keratoconus) [hypertonic saline,BCL,keratoplasty shud be deferred till edema has resolved]
- HSV /HZV keratitis[pg-20,21]
- Failed cor graft [regraft]
- ICE Sy [Artificial filtering shunts]
PROMINENT CORNEAL Ns-
- Keratoconus
- MEN type-II B
- Neurofibromatosis
- Fuch’s endothelial dystrophy
- Trauma
- Leprosy
PANNUS-
- Trachoma
- Rosacea
- CL- Tight or overwear
- Superior limbic keratoconjunctivitis
- Chem burns
SUPERFICIAL PUNCTATE KERATITIS-
- Dry eye
- Blepharitis
- Trauma
- Exposure KP
- Topical drugs [ neomycin,g’micin,preservative containing drops including artificial tears ]
- UV burns
- Chem inj
- CL
- Thygeson’s punctuate KP
10.FB under the lid
11.C’vitis
12.Trichiasis / dystrichiasis
13.Entropion / Ectropion
14. Floppy eyelid syn
T/T-
- Artificial tears without preservatives [Genteal or refresh tears]
- Cycloplegic
- Fluoroquinolone E/D
- Discontinue CL wear
NEUROPARALYTIC [ EXPOSURE] KP-
This is the result of improper wetting of the ocular surf by the tear film b/o lagophthalmos.
CAUSES-
- Facial N palsy
- Proptosis
- Eyelid scarring
NEUROTROPHIC KP-
This occurs in an anaesthetic cor→ intracellular edema→ exfoliation of epith cells & impaired epith healing→ cor ulceration
CAUSES-
- Surgery on V N
- HSV & HZV Keratitis
- DM
- Leprosy
- Acoustic neuroma
- Abuse of topical anaesthetics
- Rilay Day syn
- Congenital insensitivity to pain
CORNEAL DEGENERATION
|
CORNEAL DYSTROPHY
|
Unilateral
|
Bilateral & symmetrical
|
Peripheral
|
Central
|
No inheritance
|
Hereditary [usually AD ]
|
cor vascularisation +
|
No vascularisation
|
Middle-late life
|
Early onset
|
Sec to inflamn & systemic dis
|
No inflamn Or systemic dis
|
DYSTROPHIES-notes [J-02]
A ) ANTERIOR – Epithelium + Bowman’s membrane-
* Cogan’s microcystic
* Recurrent cor erosion syn
* Reis Buckler syn
* Meesman’s
- STROMAL-
- Granular [masson trichrome]
- Macular [Alcian blue ]
- Lattice [congo red-oil o red]
- POSTERIOR – Endothelium + DM
- cornea Guttata
- Fuch’s endothelial
- Posterior polymorphous
- CHED
Degeneration- notes
APHAKIC /PSEUDOPHAKIC BULLOUS KERATOPATHY [j-07]-case
DEF-
Corneal edema resulting from cataract extraction
PATHOPHYSIOLOGY-
Complicated cat surg→ damage & loss of endothelial cells→ remaining cells become irreg, enlarge & rearrange among themselves & then disappear→ endothelium becomes unable to pump & deturgesce the cor→ stroma begins to swell→ folds in DM & positive stromal pressure→ favours epith edema→ fld accumulation bet the basal epith cell→ blisters→ bullae
C/F-
- DOV
- Pain /discomfort
- Photophobia
- Epiphora
CAUSES-
1.Pre-existing Fuch’ dystrophy
2. PXF
3. Surgical trauma-
Mechanical-
- Endothelial touch with phaco probe ,other instrum etc
- Lens / nuclear rub against endo
- Undue long surg time
- Stripping of DM ,more with clear cor incision
Chemical-
- Irrigating fld- BSS plus is preferred. RL containing bicarbonate, reduced glutathione & adenosine protect the endo
- Intracameral drugs like adrenaline & pilocarpine containing antioxidants & preservatives→ endo damage
- VISCOAT (sodium hyaluronate + chondroitin sulphate)-protective
- Toxic subst intriduced while sterilization of instruments.
- Inadequate rinsing of instrum.(water & not saline should be used)
- Topical & intracameral anaesthesia
- Drugs causing cor toxicity-epinephrine (now preserv free),BAC preserved viscoelastic,vancomycin > 1mg/ml,inadvertent exposure of endo to 5% povidone
3.IOL-
More with-
-Iris clip IOL ( optic anterior to the iris)as they contact the endo during ocular saccades
-PMMA IOL
-Optic coming in contact with endo
-closed loop flexible AC IOL
4.Vitreous touch-
Wound leak→ vit incarceration→superior cor edema→ whole cor gets affected
5.Low grade prolonged PO iridocyclitis
6.Rise in IOP→ pushes aqueous into the stroma
PRECAUTIONS-
- Pre-oper hypotony
- Avoid endo touch by instruments
- Proper irrigating flds
- Preservative free intracameral drugs
- Regular use of visco
- Choice of proper IOL that does not come in contact with the endo
- Proper vitreous mgt
- Treat PO iridocyclitis /rise in IOP
DD-
- Post oper cor edema
- Fuch’s dystrophy
WORKUP-
- SLE—Stromal edema
-Epith edema
2. Pachmetry- central values > 590 microns asstd with irreversble cor edema
3. Specular micro-endo cell morpho
T/T-
MEDICAL-
- Ant segment inflame- Steroids + cycloplegics
- Rise in IOP-anti glauc drugs
Avoid epinephrine deriv as they cause CME
- Hypertonic agents- for epith edema-5 % NaCl E/D qid
-10 % NaCl E/O HS
4. Hydrophillic extended wear soft BCL
SURGICAL-
- Gunderson conjunctival flap
- Amniotic memb graft
- Bowman’s layer cauterization→ Dense fibrous barrier created bet stroma & epith→ fld cannot permeate into epith cells.
- Anterior stromal micropuncture
- Excimer laser phototherapeautic keratectomy
- Annular keratotomy
- PKP-Only surg that relieves pain while attempting to restore vision
- DSAEK
TRACHOMA
- Also k/as Egyptian ophthalmia
- Unhygeinic & crowded surrounding
- Spread by Conj sec- Finger, flies, & towel
CONJUNCTIVAL SIGNS-
Upper conj- Red & velvety
Follicles
Papillary enlargement
Trachomatous follicle-
- Dia-5mm
- Commence in lower fornix→ upper fornix→ row along upper tarsal margin
- Cicatrization→ minute stellate scar
CORNEAL SIGNS-
- Superficial keratitis
- Pannus-Lymphoid infiltrn + vascularization
-Vs are superficial
-Lie in epith & BM→ BM disappear→
Stroma gets inv
2 types-Progressive
-Regressive
Progressive-
Vs are parallel & vertically arranged
Cellular infiltrn extends beyond the end of NV
Regressive-
-Receding of infiltratn
-Vs extend beyond the infiltrn
HERBERT’S PITS
Follicle like infiltrates near the limbus
PATHOLOGY-
- Agent-chlamydia trachomatis serotype A,B,C
- Prokaryote, obligatory, intracellular parasite
- Present in colonies of epith cells as HALBERSTAEDTER-PROWAZEK inclusion bodies→ initial bodies→ divide & become filled with Elementary bodies→ Displace the nucleus to one side & degenerate→ cell bursts→ Elem bodies released→ attack fresh cells→ increase in size & form initial bodies
ARLT LINE-
White conj scar at the junctn of lower 3rd & upper 2/3rd of superior tarsus.
SEQUELAE- PETT
- PTOSIS- d/t dense infiltrn
- ENTROPION-Infiltrn→ scar→ contraction
- TRICHIASIS
- TYLOSIS
COMPLICATIONS-
- Corneal bacterial superinfection
- Cor ulcer
- Dry eyes
- Trichiasis
- Entropion
- Cor scarring
INV-
1.Culture of Chlamydia trachomatis in irradiated Mc Coy cells
2.Microimmunofluoresence using pooled antigens
4. IgA-IPA Light microscopy test
DIAGNOSTIC FEATURES-
- Follicles [upper >lower palp conj]
- Epith keratitis
- Pannus
- Limbal follicles & their sequelae [ Herbert’s pits]
- Stellate trachomatous scarring in the conj with linear scarring in upper tarsus.
CLASSIFICATION-
MAC CALLAN’S CLASSN
I –Incipient trachoma
- Immature follicles in upper palp conj
- no scarring
II –Established trachoma
IIA – Follicular hypertrophy predominant
IIB- Papillary hypertrophy predominant
III- Cicatrizing trachoma
- Follicles &.scarring at upper tarsal conj
IV- Healed trachoma
WHO CLASSN-
FOLLICLES-
- 5/more ,atleast 0.5mm on upper tarsal plate
- Active dis
- Needs t/t
- Conj BVs visible
INTENSE-
- Follicles & papillae so intense & numerous that more than 50 % cor BVs are not visible.
- Severe dis
- Needs urgent t/t
SCARRING-
-Tarsal conj cicatrisation with white fibrous band
-Old & inactive inf
TRICHIASIS-
-Atleast one trichiatic eyelash
-needs corrective surgery
OPACITIES-
-Corneal opacity covering part of pupillary region
-cause visual loss.
T/T-
- Topical- E’mycin / Tetracyclin e/o 5 consecutive days/month for 12 mo
- Oral-E’mycin/Tetracyclin 250-500mg qid
-Doxycyclin 100mg BD
-Clarithromycin 250-500mg BD for 3-6wks
-Azithromycin 1gm single dose
3.Pannus-no t/t
4.Trichiasis- Epilation
-Electrolysis
5.Entropion- Surgery
VIVA-
What is SAFE?
S- Surgery
A- Antibiotics
F-face wash
E- Environment
CORNEAL OPACITY-
Q- BL Corneal haze in infancy [J-07]
1 ) Congenital glaucoma-
* 1 in 10,000 births
* Isolated trabeculodysgenesis
* MC- boys
* C/F- Large eyeball
-Cor-hazy-frosted glass-photophobia
-lacrimation
-blepharospasm
-Haab’s striae
-Deep AC
-Iridodonesis
-Lens subluxation
-Axial myopia
* Rx- Goniotomy
-Trabeculotomy
-Trabeculectomy
2. Congenital hereditary endothelial dystrophy
* Focal /gen absence of endothelium
* 2 types- CHED 1- AD
-CHED 2 - AR
* Diffuse BL symmet cor edema
* Rx –PK
3. Posterior Polymorphous Dystrophy
* Endo cells display features similar to epith cells
* Onset- at birth
* AD
* 3 patterns- Vesicular
-Band like
- Geographic
* Rx- PK
4. Peter’s anomaly
* BL
* Defective neural crest cell migration-6-8 wks of fetal life
* Corneal opacity
* Bands of iris tiss adhere to the margins of opacity
* Keratolenticular adhesions
* Glaucoma-50 %
5. Metabolic abnmlities- Mucopolysaccharidoses & Mucolipidoses-
* Def of glycosidases necessary for hydrolysis of mucopolysaccharide
* AR [except Hunter’s dis- X-linked recessive]
* C/F- Facial coarseness
-Skeletal anomalies
- MR
-Cardiac anomalies
-Corneal clouding
-Pigmentary RP
-OA
-Glaucoma
6. Interstial keratitis
* Cause- Syphillis
-Tb
-Leprosy
-Mumps
-Brucellosis
-Malaria
-Allergic
C/F- Acute BL pain
-Sev blurring of vision
-Cor is hazy, lusterless & dull-ground-glass→ deep vascularisation covered by a layer of hazy cor--. Bright scarlet toned down to dull reddish pink-“ salmon patch”
Cor clears slowly from margin to centre →BVs become non-perfused-Ghost Vs
- Uveal tract profoundly inv
Rx-
1. Lubricantes
2. Topical steroids
3. Topical cycloplegics
4. PKP
5. Systemic Pn
7. Herpes simplex keratitis
-A) Primary ocular inf-skin lesion
-blepharoconjunctivitis
-Follicular Cvitis
-Sec canalicular obstrn
-B) Epith keratitis- dendritic ulcer- tapering ends with terminal end-bulbs→ enlarge→ Geographic ulcer
C) Disciform keratitis-Central zone of epith edema overlying stromal thickening + KPs + folds in DM
D) Stromal necrotic keratitis-Cheesy necrotic stroma
- Ant uveitis
-KPs
8. Sclerocornea-
- BL opacification & vascularization of the peripheral / entire cor
9. Birth trauma with forceps
UNILATERAL- Corneal dermoid
-Cor ulcer
CORNEAL OPACITY-
1. Congenital-
- Peter’s anomaly
2.Healed cor ulcer
3. Trauma
- Blunt trauma
- FB
- Penetrating inj
4.Chem burn
5. Mucopolysacharidoses
6. Cor dystrophy
7. arcus senilis.
8. Vit A def
9. Post oper- pterygium
10. Buphthalmos
Q- What is the advantage of Rose Bengal stain over Fluoresein stain?
A- Flu stains areas with absent epith, whereas RB stains infected epithelial cells surrounding the ulcer.
ARTIFICIAL TEARS / TEAR SUBSTITUTES
AIM- To increase humidity at the ocular surf & improve lubrication.
- DROPS-
- Methyl cellulose
- Polyvinylalcohol
- Sodium hyaluronate
- Sodium chloride
- Povidone
- GELS-
- Consist of carbomers
- Preferable to drops as they hav to be instilled less frequently
- OINTMENTS-
- Contain petrolatum mineral oil
- Used at bedtime
AN IDEAL TEAR SUSTITUTE-
- Forms stable tear film over ocular surface
- Lubricant property
- Shud lower surf tension of tear film→ hydrophilic layer
- Shud not interfere with tear proteins
- Shud not compromise with integrity of superficial lipid layer
- Thicken tear film
- Shud not disturb cor metabolism
- pH & surface tension shud be close to natural tears
- Long retention time
- Shud not hamper healing
CELLULOSE ESTER-
Eg- Hypromellose, Hydroxyethylcellulose, Carboxymethylcellulose
- Viscoelastic
- Increases viscosity of tears
- Good retention time
- Disadv- Useful only in Aq tear def
- Crusting of lids
POLYVINYL ALCOHOL-
- Synthetic polymer
- Good retention time
- Disadv- Blurring
POVIDINE-
- Synthetic polymer
- Co-formulated with electrolytes
- Beneficial in mucin tear def
OCULAR PRESERVATIVES
-2 types-1) Chemical
2) Oxidative
-Chemical-Alter cell membrane permeability & lyse cytoplasmic comp onents
-Eg- Benzalkonium chloride
- Chlorobutanol
- Sorbate
-Polyquad
-Oxidative-Penetrate the cell memb & interfere with cell functn
Eg- Sodium perborate
-stabilized oxychloro complex [SOC]
BENZALKONIUM CHLORIDE-
- Quaternary ammonium compd
- Used often in conjn with disodium EDTA
- Chem stable & does not degrade easily
- Effective & fast-acting against many micro-org
- Increases cor penetration of other drugs
- Adverse effects do not come until freq of use exceeds 4-6 times daily
CHLORBUTANOL-
- Alcohol based
- Anti-microbial
- Disorganizes the lipid struc of the cell memb
SODIUM PERBORATE-
- First oxidative preservative
- On contact with tear film &ocular tiss it changes into simple oxygen & water
SOC-
- Wide antimicrobial spectrum
- Destroys aspergillus niger
ADHESIVES [D-02]
- n-butyl cyanoacrylate glue
- Liquid in nature→ on polymerization→ solidifies → sticks firmly to the area of application→ Gives tectonic support
- Antibacterial
- Vasogenic
- Speeds up healing
IND-
- Impending cor perforation
- Actual cor perforation [upto 3mm]
- Cor thinning with descemetocele
- Ragged cor wounds
- Leaking cor wounds + tiss loss
- Prior to therapeautic KP in large perforation to facilitate trephination
- Temporary tarsorraphy
- Tempoary punctal & cannalicular occlusion
9. Persistent epith defect
METHOD-
- Topical anaesthesia with lid block→ Avoid compressive actn of orb oculi wen pt squeezes
- Lid separation with wire speculum
- Preparation of area of application-
- remove all dead & devitalized tiss & epith from the margin of perforation to abt 1- 1.5mm with no 15 blade
- Dry the area with a surgical spear [Very imp as glue will not stick to wet surf]
- Sometimes aq keeps leaking. So aq shud be completely milked out by gentle pressure
- Application of glue-
- Remove a few drops of glue from the ampoule with a tuberculin syringe
- Put it on a dry surf
- Dip a smooth , dry metal rod in the glue drop
- Transfer it immediately to the area of application by placing the rod perpendicular on the surf.
- Press the rod gently
- Remove it instantaneously
- Pt shud keep the eye still to avoid spillage
- bandage contact lens
- Put a large size [14mm], flat [ 8.6-9mm base-curve] & low water content BCl
- Remove the speculum
- AC can be seen reformed if it is a fresh perforation before removing the spec.
- Postoperative-
- After 1 hr, check pos of glue,adequacy of glue, centration & movt of lens & reformation of AC
- Broad spec antibiotic
- Again see after 24 hrs
- Avoid premature removal
- It takes 6-8 wks for the glue to loosen.
- After 6-8 wks remove it gently with a fine forcep
- Any part which has not loosened shud be left in place
- Forceful attempt to remove it→ reperforation
- COMPLICATIONS-
- Cataract
- corneal infiltration
- glaucoma
- giant papillary c’vitis
- Retinal toxicity
- granulomatous keratitis
- symblepharon
PENETRATING KERATOPLASTY
INDICATIONS-
1.Bullous KP [aphakic & pseudophakic]
2. Fuch’s endo dystrophy
3.Keratoconus
4.Failed previous transplant
5. Stromal cor dystrophy
6.Corneal opacification foll-Keratitis[bacterial,viral &fungal]
7. cor degeneration
8.Mechanical injury
9.Chem burns
10.Immune mediated cor dis & perforation
INDICATIONS IN CHILDREN-
- Congenital cor opacities-
- Peter’s anomaly
- Sclerocornea
- Glaucoma with cor edema
- Cor dystrophy
- Trauma
- Non-traumatic-
- Infections
- Steven Johnson syn
- Keratoconus
EVALUATION OF DONOR CORNEA BY
SPECULAR MICROSCOPY-
Features of an unsatisfactory cornea-
1.Endo cell count < 1500cells/ mm2
2.Polymegathism /Pleomorphism
3. corneal guttate
4.Extensive areas with severe edema
5.Inflam cells on endo
CORNEAL PRESERVATION- [J-03,J-04]
A] SHORT TERM STORAGE
1} MOIST CHAMBER METHOD-
* Whole globe preservation with saline humidification
* 4deg c for 48 hrs
* ADV- inexpensive
-easily transportable
-min manipulation
* DISADV- storage time is short,so surgery has to be performed as an emergency.During this time it is diff to perform HLA typing & screening for HIV & hepatitis.
B] INTERMED TERM STORAGE-
1} Mc Carey –Kaufman medium-4 deg C for 4 days
1) TC 199
2) Dextran 5%
3) Bicarbonate buffer
4) Pn & gentamicin
* Modified MK medium-
- Buffer- 0.025 M HEPES
- pH indicator- phenol
2} K-sol medium
3} Corneal storage medium [CSM]
4}Dexol medium
5}Optisol med
C] LONG-TERM STORAGE-
1} Organ –culture medium-35days
* Components-
1) Eagle’s min essential medium
2) Earle’s salt without L-glutamine
3) L-glutamine
4) Decomplemented calf serum
5) Chondroitin sulphate 1.5 %
* The corneoscleral segment is placed in Petri dish containing 15ml of the medium with the endo side up for 2-3 days for one or two medium changes.
* Stored at 34 deg C in 5 % CO2
* Cor are then suspended in 130ml of the medium by a special hook inserted thru the scleral rim & then stored at 34 deg c
* Bottle is examined daily for contamination
* If no growth seen for 10 days ,med considered sterile
2} Cryopreservation-1year
* Corneoscleral rim is passed thru a series of sol containing increasing conc of dimethyl sulfoxide [DMSO] upto 7.5 %
* Tissue is placed in each sol for 10 min
* next the tiss is frozen upto -80 deg c
* Stored at -160 deg C indefinitely
SURGICAL TECH
1. ANAESTHESIA- LA- PBB
2. FIELD PREP-
-Plastic drape-isolates eyelashes & meibomian gld orifices
-Conj sac rinsed with BSS
3. EYE EXPOSURE-
-Wire speculum & bridle suture
-Flieringa scleral ring- to prev scleral collapse
4. TREPHINING OF RECIPIENT BUTTON-
- 7.5 – 8.5mm size
-Proper centering-critical step
-Trephine is rotated giving equal pressure over the cor, cutting 80 % depth
-Types- 1) Motorized T – less stromal disruption & smoother interface
2) Suction- fixation T –Hessburg-Baron Trephine
-Outer cor suction ring for fixation & inner circular cutting blade
-Allows measured depth penetration
-Each revolution advances the blade by 250 micron
5. AC ENTRY & CORNEAL BUTTON REMOVAL-
-AC may be entered with the trephine producing a perpendicular cut & easy removal of cor.Chance of iris & lens injury are high
-AC may also be entered wuth a sharp blade.Cor buttin is removed with corneoscleral scissor
-Posterior tags of stroma & DM shud be removed to avoid tilting of graft & astigmatism
6. LENS MGT-
- Cat shud be removed at the time of KP as cat progresses more rapidly & later on removal leads to graft endo damage
7. VITREOUS MGT-
-An intact vit face shud be preserved
-Any vit in front of iris shud be removed with Vanna’s scissor or sponge
-Host-graft shud be totally free of vit
8. TREPHINATION OF DONOR COR-
-Donor cor is immersed in Gentamicin0.3 % E/D in a bowl for 20min
-CB is gently teased away from the scleral spur & iris-lens diaphragm freed from cor
-AC collapse shud be avoided
-Cor.scleral button is transferred to a Teflon block endothelium up
-Trephine is used to cut the graft
-Graft-same size-myopia
-0.2mm larger in phakia
-0.5mm larger in aphakia,pseudophakia,& lens exchange
9. GRAFT PLACEMENT & AC MAINTENANCE-
-Visco is placed on iris & ant lens capsule
- Donor button is transferred to recipient bed
10. CORNEAL BUTTON SUTURING-
- First 4 sutures- Cardinal sutures
- 1st placed at 12o ‘clock→ 6 o’clock
-Equal distribution of tissue on both sides of suture
- 3 & 9 o’clock
-10-o nylon
-Each bite-1mm long in the donor & 1.5mm long on the recipient side
-INTERRUPTED SUTURE-
* Preferred in
- childn,
- vascularized cor,
- uneven thickness,
- localized inflamn
* Drawback-stim more inflame & vascularization
* Adv- Easy to apply & remove
-Rapid wound healing
-CONTINUOUS SUTURES-
* Used – no vascularization
- Even thickness of graft & rim
- No inflamn
* Adv- less inflamn
-uniform wound healing
-Ease of intraoper suture loop tension adjustment
* Disadv-Cannot be selectively removed
-If one breaks , entire suture may be affected
COMPLICATIONS- [LQ]
EARLY-
- Primary graft failure-
Irreversible graft edema in the immediate PO period
Rx –regraft
- Glaucoma-
causes of raised IOP-
- Collapse of TM→obstructs aq outflow
- Pre-existing glauc
- PO inflame
- Visco retention
- Malignant glaucoma
- Steroid induced glauc
Use of oversized grafts in aphakic / pseudophakic eyes→ less angle distortion→ less incidence of glauc
Rx –Routine glauc t/t
- Epithelial defect
Rx-
- Patching & BCL
- Lubrication
INTERMEDIATE-
- Graft rejection-4 types SHORT NOTE
A] Epithelial rejection-seen as an elevated rejection line
B] Subepithelial infiltrates
- KRACHMER SPOTS
-reminiscent of adenoviral keratitis
-seen below bowman’s mem as white infiltrates
-0.2-0.5mm dia
C] Stromal rejection
-peripheral full-thickness haze with CCC
D] Endothelial rejection-KHODADOUST LINE-seen in a vascularized area of peripheral donor cornea or at a point of junction of anterior synechiae with endothelium
- Graft infection-HSV & acanthamoeba keratitis
3 sources of infection-
A ]donor contamination
B]incomplete excision of recipient infected tissue
C] ambient air
- Wound dehiscence-
-Always at the graft-host junction
Rx- patching
-BCL
-Aq suppressant
-consider resuturing if leak .>. 3 days
LATE-
- Recurrence of disease-Reis Buckler
-Granular dyst
-Lattice dys
-Macular dys
-HSV keratitis
2. Late graft failure of unknown etio
3.Post KP astigmatism
See –Graft failure from notes
PERSISTENT EPITHELIAL DEFECT
Causes-
1.Trauma-
-Chem/thermal inj
Radiation inj
Fingernail inj
Cor FB
Postsurg
2.Inflam-uveitis
-marginal keratitis
3.Deg & dystrophy-
-Meesman’s d
-Reis Buckler d
-Stromal d
-Fuch’s d
4.Neurogenic- HSV & HZO
5.Nutritional –vit A def
6. Iatrogenic- Drugs
-CL
7.DM
EXAM-
-Fluorescein dye[1 %] stain-delineates area of epith loss
-Denuded area-brilliant green
Rose Bengal dye 1%-Stains SPK
Stains dead & devitalized cells
-Dimension of epith def is measured under SL in sqmm
-Plannimetry-
* Cor is stained with Flu dye & photographed using fundus/ant seg camera with a blue filter
* Area of def & the cor is calculated & size expressed as % of the total cor area.
MGT-
A] Medical line-
1. Topical antibiotic e/o
2. Topical fibronectin-prev dessication & frictional damage to migrating epith sheet by lid movts
NO PLACE FOR STEROIDS
3. Topical cyclplegics
4. P&B-
ADV-Promotes epith healing
-Immobilizes lids→ lessens trauma to epith→ symptomatic relief
DISADV- Decreases oxygenation→slows epith migration & proliferation
-Increases cor temp→ bact growth
B] BANDAGE SOFT CONTACT LENS-
IND-Recurrent cor erosions
-large cor abrasion
COMPLICATIONS-Cor edema, vascularization & infection
COLLAGEN SHIELD-
- Alternative to BCL
- Fabricated from porcine scleral tiss containing typeI & III collagen
- Dia-14.5mm
- Radius of curvature-9mm
- Thickness-0.1mm
- Dissolves over 12-72 hrs & needs replacement
- ADV over CL-
-Conforms to cor contour & eliminates fitting prob
-Biodegrades with time & hence increases O2 transmission
-Speeds re-epithelization
-Preferred in only seeing eye & CL wearers
DISADV-
-Excessive movt→ dislodges into fornix
-Cost factor
TISSUE ADHESIVES-pg 44
C] SURGERY-
CONJUNCTIVAL GRAFT-
-Abnml conj 5mm posterior to limbus resected for 360 deg
-Total superficial keratectomy done
-3mm conj taken from fellow eye & sutured on cor periphery with 10-0 monofilament.
GUNDERSEN FLAP-
-360deg peritomy
-Cor is covered with coj & sutured inferiorly to inf limbal conj edge & superiorly to episclera
-Superior conj is left bare which covers by rapid epitheliazation
LIMBAL ALLOGRAFT STEM CELL TRANSPLANTATION
TARSORRHAPHY
AMT
RECURRENT PTERYGIUM
T/T-
- MC RENOLD’S TRANSPLANTATION-
Head of the pterygium is dissected from the cor & transplanted beneath the lower bulbar conj
2.BARE SCLERA TECH-
After excision of pterygium, a small area of sclera in relation to the affected cor is not covered by the conj but thoroughly denuded of SC tiss & allowed to heal by granulation tiss.[
- CONJUNCTIVAL AUTOGRAFT
u can very well explain
4.LAMELLAR KP
5 BETA IRRADIATION-on 2nd or 3rd PO day
6 THIOTEPA 1:2000 sol 6 hourly for 6weeks
7 MMC –E/D 0.4mg/ml [0.04%]
8 ARGON LASER