

ORBIT
VOLUME- 30 ml
WALLS OF ORBIT-
MEDIAL WALL –
1.body of sphenoid
2.Frontal process of maxilla
3.Orbital plate of ethmoid
4.Lacrimal bone
Applied Anat-
1 Thinnest bone→Ethmoiditis→orbital cellulites
2.Easily eroded by inflamn,cysts & neoplasms
3.Easily # d
4.H’age [ethmoidal Vs]
FLOOR-
Triangular
3 bones-Medially-Maxilla
-Laterally-Zygomatic
-Post-Palatine
AA-
- Blow out #- MC inv
- Maxillary antrum tum
LATERAL WALL-
Anteriorly- Zygomatic
Posteriorly- Greater wing of sphenoid
Ant-* Zygomatic groove & foramina
*Lateral orbital tubercle of Whitnall→check ligament of LPS
Post-Spina recti lateralis-LR
AA- Zygomaticosphenoid suture- Imp landmark for Kronlein’s proc
ROOF-
- Orbital plate of Frontal
- Lesser wing of sphenoid
Fossa for Lacrimal gld
AA-
1.Periorbita easily peels away.Therefore a sharp object can penetrate the roof & damage the frontal lobe
2.Not perforated by Ns/Vs.Therefore easily nibbled in transfrontal orbitotomy
APEX OF ORBIT
- Post end of orbit
- 4 walls converge here
- 2 orifices-optic canal
- -superior orbital fissure
- OPTIC CANAL-connects orbit to mid cranial fossa
-transmits-Optic N
-Ophthalmic A
-UL enlargement on x-ray-ON glioma &
Meningioma
-Length-6-11mm
- SUPERIOR ORBITAL FISSURE-
-Length-22mm
-Comma shaped
-Bounded by greater & lesser wings of sphenoid
-Transmits-
Upper part-Lacrimal N
-Frontal N
-Trochlear N
Middle part-2 div of III N
-Nasociliary N
-VI N
Lower part-Inf ophthalmic V
TENON’S CAPSULE [Fascia bulbi]-
- Envelopes the globe from limbus to optic disc
- Inner surf is in contact with the sclera & connected by fine trabeculae
- Outer surf is in contact with orb fat post,& subconj tiss ant
- Seperated from sclera by episcleral space
- Lower part is thickened-Hammock-on which the globe rests-K/as Suspensory ligament of Lockwood
- Pierced by-ON
-Ciliary Vs & Ns
-venae vorticosae
-EO ms
ORBITAL SURGICAL SPACES-[D-03]
1.Subperiosteal space
2.Peripheral space
3.Central Space
4.Tenon’s space
SUBPERIOSTEAL SPACE-
Bet the orbital bone & periorbita
Lesions-
- Dermoid cyst
- epidermoid cyst
- mucocele
- subperiosteal abscess
- myeloma
- osteoma
- fibrous dysplasia
- sphenoid wing meningioma
- aneurysmal bone cyst
- haematoma
- cholesteatoma
- eosinophilic granuloma
PERIPHERAL SPACE- [extraconal]
- Bet the periorbita & the fascial septa that interconnect the EO ms
- Eccentric proptosis
- Lesions-Capillary haemangioma
-Pseudotum
-Malignant lymphoma
-Rhabdomyosarcoma
-Intrinsic neoplasm of lacrimal gld
Surgical approach-Anterior & Lateral orbitotomy
Contents-
- Peripheral orbital fat
- Ms-LPS, SO, IO
- Ns-Lacrimal N
-Frontal N
-Trochlear N
-Ant ethmoidal N
-Post ethmoidal N
* Vs-Sup ophthalmic V
-Inf Ophthalmic V
Lacrimal gld
Half of Lacrimal sac
CENTRAL SPACE [Intraconal/ Retrobulbar]
- Bounded ant by the tenon’s capsule & peripherally by the EO ms & their intermuscular septa.
- Post it is continuous with the peripheral space
- Axial proptosis1)Cavernous haemangiom
- 2)ON Glioma
3) -ON meningioma
4) -orbital cellulites
5) -cavernous sinus thrombosis
6) -pseudotum
7) -TED
8) -schwanoma
9) -neurofibroma
10) -neurolemoma
11) -AV malformation
Surgical approach-Lateral o’tomy
CONTENTS-
- 4 Ns- Optic N
-III N
-VI N
- Nasociliary N
- Ciliary ganglion
- Ophthalmic A
- Superior oph V
- Orbital fat
SUBTENON’S SPACE
- Potential space around the eyeball bet the sclera & tenon’s capsule
- Pus collected in this space is drained by incision of tenon’s capsule thru the conj
PAINFUL PROPTOSIS-[ D-02]
- pseudotumour
- TED
- orbital cellulites
- Cavernous sinus thrombosis
- orbital h’age
- Adenoid cystic Ca –lacrimal gld
- Ca- nasopharynx
- metastasis
- lymphangioma
NON-AXIAL PROPTOSIS-
* Down & medial-Dermoid
-Lacrimal gld tum
* Down & out-Frontoethmoidal mucocele
* superior-Maxillary sinus tum
-mucocele
* cysticercosis
PSEUDOPROPTOSIS-
- High myopia
- cong glaucoma
- craniosynostosis
- C/L-microphthalmos
- “ -pthisis
- “ -enophthalmos
7.” -ptosis
8. staphyloma
PROPTOSIS-passive protrusion of the globe from the socket
EXOPHTHALMOS-active protrusion of the globe
LID RETRACTION-
1.TED
2.Duane;s lid retraction syn
3.Aberrant regeneration of III n
4.Midbrain lesion
5.Multiple sclerosis
6.Hydrocephalus
7.Meningitis
8.Parkinson’s dis
9.Marcus Gunn Jaw winking syn
10.Lid scarring
PULSATILE PROPTOSIS-
1.Transmitted vascular pulsation
* carotid cavernous fistula
* saccular aneurysm of ophthalmic A
2.Transmitted CSF pulsation
* congenital absence of orbital roof-Meningocele
-Encephalocele
* Erosion of orbital roof-Dermoid
-neurofibromatosis
ENOPHTHALMOS-
Recession of the globe within the orbit
1.Microphthalmos
2.pthisis
3.Horner’s sy
4.Abscence of greater wing of sphenoid [neurofibromatosis]
5.Blow out # orbital floor
PSEUDOENOPHTHALMOS-
- microphthalmos
- phthisis bulbi
UNILATERAL PROPTOSIS- [D-01]
1.Orbital cellulites
2.Pseudotum
3.cavernous sinus thrombosis
4.A-V aneurysm
5.orbital h’age
6.orbital emphysema
7.orbital tum
BILATERAL PROPTOSIS
- cav sinus thrombosis[later]
- Empyema of accessory sinus of nose
- lymphoma
- pseudoleukemia
- oxycephaly [Tower skull]
- leontiasis ossea
- TED
PROPTOSIS IN CHILDREN-
1.Dermoid [UL]-25
2.Epidermoid [UL]
3.ON glioma[UL]-29
4.RB [initially UL]
5.rhabdomyosarcoma [UL]-33
6.Leukemia-granulocytic sarcoma [chloroma] [BL]
7.Neuroblastoma [BL]-
-arises from primitive neuroblast of sympathetic chain in abdo,thorax & pelvis.
-BL metastasis
-abrupt proptosis
-sup orb mass
-lid ecchymosis
8.Plexiform neurofibromatosis
9.Capillary haemangioma [UL]-26
10.Lymphangioma
11.orbital cellulites [UL]-18
DYSTOPIA-
- Displacement of the globe in the coronal plane d/t extraconal orbital mass such as lacrimal gld tum.
- Horizontal displacement is measured from the midline [nose] to the nasal limbus.
- Vertical dystopia is read off a vertical scale placed perpendicular to a horizontal rule placed over the bridge of the nose.
EVALUATION OF PROPTOSIS
HISTORY-
- Age of onset
- Nature of onset-sudden-orb emphysema
-orb cellulites
-RB h’age
-Cav sinus thrombosis
Gradual-Benign
-Pseudotum
3. Duration-longstanding
-short duration
4.Progression-slow
-rapid
5.symptoms-
* pain-inflam &inf
-cor inv [exp keratitis in TED]
*diplopia-myositis,TED
*decreased v/a-cor inv
-ON inv
-induced hyperopia
6.Lid malposition-Lateral ptosis of UL-lacrimal gld
-UL ptosis d/t interference of LPS-sup orb tum
-Lid retraction-TED
ORBITAL EXAM-
OCULAR-
- Vision-reduced-exp KP
-compressive optic neuropathy
-choroidal folds at macula
2.pupil-RAPD
3.EO movts-limited-useful in localizing orbital lesion
4.SLE-Status of cor- for Exp KP –proptosis
_lid retraction
-Large tortuous veins-Indirect CCF
5. RESTRICTIVE VERSUS NEUROLOGICAL OPHTHALMOPLEGIA-
1] Forced Duction test
* Topical anaesthesia
* Insertion of a ms in the involved eye is grasped with a forcep & the globe is rotated in the dir of limited ocular mobility.
2] Differential .IOP test- IOP in prim pos& then in the dir of limited motility
Interpretation-
- >6mm-resistance transmitted to globe b/o ms restriction
- < 6mm-neurological lesion
6. Fundus-Disc edema
-OA
-shunt Vs on disc-[Optociliary shunts]-Meningioma
-Glioma
-Cavernous
haemangioma
-choroidal striae-mass indenting globe
-TED
-mucocele
7. Colour vision-optic N dysfunction
8 .Visual fields
LOCAL EXAM-
- INSPECTION-True /pseudoproptosis
-UL/BL
-Facial proportion & symmetry
-Axial /eccentric
-visible pulsation
-colour-errhythema-inflamn
-bruising-trauma
2.PALPATION-
* orbital margins
* insinuation of finger
* retropulsion of globe
* orbital thrill
* swelling around eye
* regional LN
* sensation
3AUSCULTATION-Bruit- CCF
-AV malformn
Best heard with the bell of stetho.
4.TRANSILLUMINATION-for ant cystic lesion
5.EXOPHTHALMOMETRY-
Measurement from cor apex to lat orb margin
Normal-< 22mm
Diff bet 2 eyes > 2mm-significant
Mild- 21-23mm
Mod- 24-27mm
Sev - >28mm
METHODS-
- Simple transparent ruler
- Clinical Nafzaeger’s method-Examiner stands behind the pt & turns the pt’s head straight down the nose.He then rotates his head backwards until he can just see the apex of the cor.If he sees one apex more, then it is proptosed
- Hertel’s e’meter-measures BE simultaneously
- Leude’s e’meter
6.Systemic exam-For thyrotoxicosis
-prim tum →sec in orbit
7.Nasal exam-nasal & sinus inf &inflame
INVESTIGATIONS-
- PLAIN X-RAY
Water’s view-Orbital floor #
-maxillary & ethmoid sinus
Caldwell’s view-Superior orb fissure
-Frontal & ethmoidal sinus
Rhese view-Optic foramen
Lateral view- Nasopharynx
X-RAY SIGNS-
Enlargement of orbit-ON glioma
-haemangioma
-rhabdomyosarcoma
-dermoid
Increased bone density-meningioma
-fibrous dysplasia
-Paget’s dis
-osteo-blastic metastasis
Decreased bone density-malignant tum
Intra-orbital calcification-RB
-IO varix
-ON meningioma
Superior orbital fissure enlargement-Infraclinoid carotid
Aneurysm
-Intracavernous aneurysm
Optic canal enlargement-ON glioma
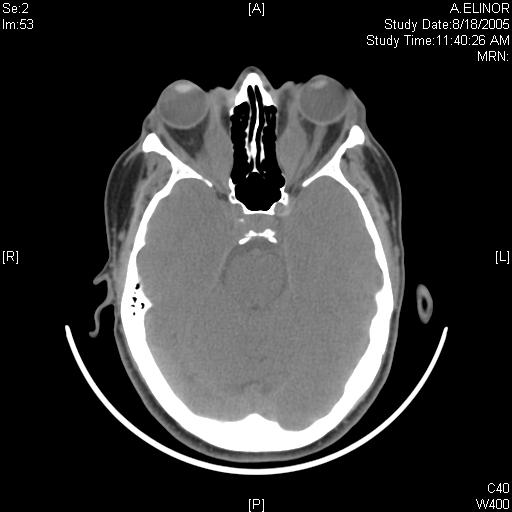
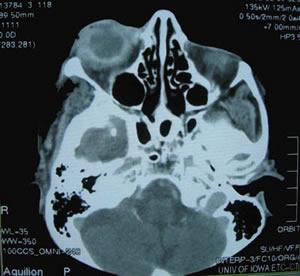
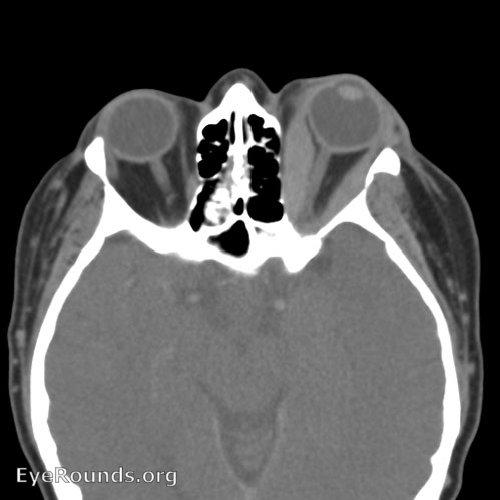
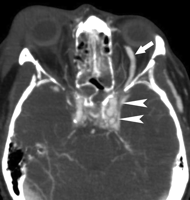
2.CT SCAN-
LESIONS | FINDINGS |
ON glioma | Fusiform enlargement of ON & canal |
ON sheath meningioma | N/enlarged ON with more density peripherally & less density centrally-TRAMTRACK SIGN /DOUGHNUT SIGN |
Cavernous haemangioma | Well circumscribed mass with marked contrast enhancement |
Cav sinus thrombosis | Enlarged sup oph V |
Pseudotum | EO ms belly & tendon thickened |
TED | Only ms belly inv-COKE-BOTTLE |
3.USG
4.MRI-Bones not well delineated
-best for detection of IO part of ON & intracranial extension
T 1- black
T 2 -white
5.Invasive procedure-
1. Orbital venography-For orbital varix
2.Carotid angiography-For pulsating exophthalmos
H/P-FNAB for suspected orb metastasis
THYROID EYE DISEASE
- Autoimmune dis
- 3rd -4th decade
- F > M
- Ophthalmic Grave’s dis/euthyroid Gr.dis-
Occurrence of signs of Grave’s dis in a pt who is not clinically hyperthyroid
- UL or BIL
- Triad of Grave’s dis-Eye signs
-Thyroid acropachy
-Pre-tibial myxedema
PATHOGENESIS
- Inflammation of EO ms-
-Pleomorphic cellular infiltr
-Increased glycosaminoglycans
- Osmotic imbibition of water
All these cause ms enlargement→ON compression
→Ms degeneration→fibrosis→
Restrictive myopathy→
Diplopia
2.Inflam cellular reaction-
Infiltration of interstitial tiss,orb fat & lacrimal gld with lymphocytes,plasma cells,macrophages & mast cells
+ Increased glycosaminoglycans + Retention of fld→Increased orb content vol→rise in IOP
C/F-
1.Soft tiss inv
2.Lid retraction
3.proptosis
4.optic neuropathy
5.Restrictive myopathy
1.SOFT TISSUE INV-
SYMPTOMS-
- Grittiness
- Photophobia
- Lacrimation
- Retrobulbar discomfort
SIGNS-
- Periorbital & lid swelling
- Conjunctival & episcleral hyperaemia
- Chemosis
- Superior limbic keratoconjunctivitis
- Keratoconjunctivitis sicca
2.LID RETRACTION-
PATHOGENESIS-
- Fibrotic contracture of LPS & IR
- Fibrosis of IR→ Sec overaction of LPS-SR complex→Lid retraction from downgaze to upgaze
- Fibrosis of SR→Sec overaction of IR→ Retraction of LL
- Increase thyroid hormone→Sympathetic stim of muller’s ms→lid retraction
Lid signs-
1.VON GRAEFE’S SIGN-Lid lag
2.DALRYMPLE’S SIGN-Lid retraction
3.STELLWAG’S SIGN-Infrequent blinking
4.MOBIUS SIGN-Insufficient convergence
5.KOCHER’S SIGN-Staring look
Rx-2-5 % guanethedin E/D
-orbit→ squint→ lid
-IR RECESSION
-Mullerotomy
-Recession of LL retractors + scleral graft
3.PROPTOSIS-
* Axial
* UL/BL
* symmetrical/asymmetrical
*Exposure KP→corneal ulcer
T/T-
- If rapidly progressive & painful proptosis during the congestive phase-Oral Prednisolone 60-80mg/day
- for compressive optic neuropathy-IV methyl prednisone 0.5gm in 200ml isotonic saline over 30 min
- Radiotherapy-Supervoltage radiation-Total 2000 rads [200 rads/day for 10 days]
- Combined therapy-
-Irradiation
-Azathioprine
-Low-dose steroid
5.Surgical decompression-2-wall
-3-wall
-4-wall
2-wall-Antral-ethmoidal
-Part of floor +post portion of medial wall
-3-6 mm of retroplacement
3-wall-Kronlein’s -Antral-ethmoidal decompression
+
Removal of lateral wall
6-10mm retroplacement
4-wall-3-wall decompression + removal of lat ½ of roof
+ Large portion of sphenoid at the apex of orbit
-10-16mm of retroplacement
4.OPTIC NEUROPATHY
PATHOGENESIS-
Congested & enlarged recti→compression of On & its bld supply at the orbital apex
C/F-
- impaired central vision
- RAPD
- Colour desaturation
- Reduced light brightness
- Field defect-central/paracentral scotoma
- Optic disc-N
-swollen
-atrophic
T/T- IV methylpred→ orbital decompression
5.RESTRICTIVE MYOPATHY-
* Elevation defect [fibrotic contracture of IR]
* Abduction defect[ - “ - MR]
*Depression defect [ - “ - SR]
* Adduction defect [ - “ - LR]
T/T-
1.IND -Diplopia in prim / reading pos
-Dis shud be stable for 6 mo
Tech-
-Recession of IR /MR on adjustable sutures
2.Botulinum toxin inj into inv ms
Werner’s class of severity of o’pathy-NO SPECS
N- no S/S
O-Only signs-lid retraction
S-Soft tissue inv
P-Proptosis
E-EO ms inv
C-Cor inv
S-Loss of sight
INVESTIGATIONS –
- THYROID FUNCTION TESTS-
- Thyroid stimulating hormone [ TSH]
- Serum T3 & T4
- Thyrotropin releasing hormone [TRH]
- Thyroid antibodies-TSH-receptor antibodies [TRAB]
-Antimicrosomal antibodies
-Antithyroglobulin antibodies
2.CT SCAN-Enlargement of belly of EO ms with sparing of tendon-coke bottle
3.USG-
* can detect early ms inv without clin signs
* assessment of ON compression at the orbital apex
DDs-
- III Npalsy with aberrant reg
- UL may elevate with downward gaze ( pseudo-von Graefe sign.
- Limited OM
- Parinaud’s syn-
- lid retraction
- Limited upgaze
- Mildly dilated pupil reacting poorly to light with intact near reflex.
ORBITAL CELLULITIS
DEF-
Life-threatening infection of the soft tiss behind the orbital septum
EPID-
- Mc in childn
- Org-Strepto. Pneum
- Strepto pyog
- Staph aureus
- H.inf
CAUSES-
- Ethmoidal sinusitis-thru the thin med wall
- Extension of preseptal cellulites thru the orb septum
- Local spread from- dacryocystitis,mid-facial or dental inf via maxillary sinusitis
- Haematogenous spread
- Post-traumatic-within 72hrs of an injury that penetrates the orb septum
- Post-surgical-ret,orb,lacrimal
- Subperiosteal abscess,stye & furunculosis
CLINICAL FEATURES-
SYM-
- malaise
- fever
- pain
- visual impairment
SIGNS-
- UL
- Tender,warm ,red,woody hard periorbital & lid edema
- Marked chemosis
- RAPD
- Proptosis-lateral & down
-reducible
* Painful O’plegia
* Diplopia
* ON dysfunction→ reduced vision
COMPLICATIONS-
- Ocular-
- Exposure KP
- Raised IOP
- CRAO /CRVO
- Endophthalmitis
- Optic neuropathy
2.Intracranial-
* meningitis
* brain abscess
*cav sinus thrombosis
3.Subperiosteal abscess-mc along medial orbital wall
4.Orbital abscess
5.Papilloedema
6.Exud RD
7. Panophthalmitis
INV-
- LAB-
-Bld count-TLC, DLC
-Leucocytosis > 15000
-Bld culture-Purulent material collected from nose with a cotton swab or calcium alginate swab→ Gram stain→ cultured on aerobic & anaerobic media
-ESR
-Antistreptolysin O [ASO] titre-raised [for alpha haemolytic strepto]
2. USG-Location of orbital FB & abscess
3. CT scan-diff bet sev preseptal & orbital cellulitis
- PNS-Blurred osseus margin
-air fluid level
-inflamed tiss within aerated sinus


4 . LP- meningitis
T/T
1.Antibiotics-
-< 4 YRS-
1]cefotaxime -80-120mg/kg/day qid
2]cefuroxime- 75-150mg/kg/day tds
Adults-
1] Cefuroxime- 750-1.5g/kg 8hrly
2]ceftriaxone 1-2 gm/day
2. Anti-inflam & analgesics
2.Ind for surg-
* unresponsive to antibiotics
* Decreasing vision
* Orb / subperiosteal abscess
* Atypical picture which may merit diagonistic biopsy
* increasing proptosis
* EO motility defect
3.Intracranial abscess-neurosurgical drainage
ON function should be tested for spread into cav sinus
DIFF BET PRE-SEPTAL & ORBITAL CELLULITIS-
Pre-septal-
- Nml V/A
- Nml OM
- Nml pupillary reactions
PSEUDOTUMOUR
- Also k/as Idiopathic orbital inflammatory dis
- Non-neoplastic
- Non-infectious
- Space occupying orbital lesion
- Unilateral-adults
- Bil-child
- M > F
- 3rd -6th decade
H/P-Pleomorphic cellular inflame infiltration foll by reactive fibrosis
AETIO-
- Spread of inf from-PNS
-Dacryocystitis
-Chr osteomyelitis
-Dental inf
2.Granulomas-
Non-specific-Trauma
-Retained IOFB
-Cholesteatoma
-Rutured dermoid cyst
Specific-Tb,Syphyllis
3.Fungal-Aspergillosis
-Mucormycosis
4.Ectopic lacrimal gld tiss in orbit
SYMPTOMS-
- acute redness
- swelling
- pain
SIGNS-
- Decreased V/A
- Lid edema
- chemosis
- proptosis
- Painful O’plegia
- Fundus-papilloedema
-exud RD
COURSE-Sev prolonged inflamn→Fibrosis of orbital tiss→ FROZEN ORBIT \
-ptosis
-O’plegia
-visual imp caused by ON inv
INV-
1.CT scan-enlarged tendon & belly of ms

2.USG-diffuse heterogenous infiltration
3.Bld tests-
* ESR
* CBC
* ANA
* BUN
* S. Creatinine {vasculitis ]
*B sugar
* ANCA [Weg gr]
* ACE Assay- sarcoidosis
* Gallium scan-Sarcoidosis
4. Biopsy- to r/o neoplasia & confirm diagnoses
T/T-
1.Sys steroids-60-80mg/day
2.Radiotherapy-10 Gy
3.Cyclophosphamide-200mg/day
TOLOSA HUNT SYNDROME
DEF-
Non-specific granulomatous inflamn of cav sinus, SOF,orb apex
Recurrence & remissions
C/F
- Diplopia
- Ipsilateral periorbital / hemicranial pain
- Proptosis
- III,IV,VI,V[1 & 2 div] palsies
- V n-oph div –Hypesthesia & decreased cor reflex
- Visual field & V/A- Nml
- Pupils relatively spared
T/T-sys steroids + antibiotics
CAROTID CAVERNOUS FISTULA
[J-2004]
DEF-
An abnormal communication bet the carotid A & cavernous sinus
TYPES-
1} DIRECT CCF
* 70-90%
* high flow shunt
* Carotid A bld passes directly into cav sinus thru a defect in the intracavernous part of ICA
* Results from-
1] Trauma-Basal skull #
2] Spontaneous rupture of an intracav carotid aneurysm or atherosclerotic A.
-Postmenopausal women
-low flow rate
C/F-
Classic triad-Pulsatile proptosis
-Conj chemosis
-Flushing noise in head
SIGNS-
- Ptosis
- Chemosis
- Pulsatile proptosis
- Bruit
- Thrill
- Raised IOP
[d/t raised episcleral venous press &orb congestion]
- Ant segment ischaemia-cor epith edema,aq cells &flare,iris atrophy,cataract,rubeosis iridis
- O’plegia-III, IV , VI n [VIn MC inv d/t its free location in cav sin]
- Fundus-optic disc edema,venous dilatation,intraret h’ages
INV-
- CT scan- show- Prominent sup oph vein
MRA shows prominent sup oph v
T/T-
IND-
- Sec glaucoma
- Sev Proptosis
- Intractable bruit/ headache
- Diplopia
- Ant seg ischaemia
- Exp KP
Interventional Radiology-
-Detachable balloon occlusion of fistula
-Balloon is introduced into the cav sinus thru➔
* tear in the ICA or
* inferior petrosal sinus or
* sup oph vein
- INDIRECT CCF-
-Intracav portion of ICA remains intact
-communication bet-
1. Meningeal br of ICA & the cavernous sinus
2. - “ - ECA - “ -
3Meningeal br of both ICA & ECA & the cavernous sinus.
CAUSES-
- Congenital malformation
- Spontaneous rupture
C/F-
- Dilated conj & episcleral Vs
- Exaggerated ocular pulsation
- Raised IOP
- Proptosis-mild
- Bruit
- O’plegia [VI N palsy]
- Fundus- NML or mod venous dilatation
T/T- Interventional radiology
DERMOID CYST-spot
DEF-
Benign cystic teratoma [choristoma ] derived from displacement of ectoderm to a subcutaneous location along embryonic lines of closure.
PATHOLOGY-
- Lined by keratinized stratified squamous epithelium
- Fibrous wall
- Contain dermal appendages [sweat glds, sebaceous glds,hair follicles]
- Epidermal cysts do not contain such appendages
TYPES-
1.Superficial
2.Deep
SUPERFICIAL DERMOID-
- anterior to orbital septum
- Presents in infancy
- Painless nodule
- Mc –superotemporal quad
- SiGNS-Firm,round, smooth, non-tender mass
-freely mobile
-post margins are easily palpable denoting lack of deeper extension
T/T-
Excision in toto, taking care not to rupture the lesion,since leaking of keratin into the surrounding tiss may cause sev granulomatous reac
DEEP DERMOID-
- Presents in adolescence /adult life
- Signs-Proptosis
-dystopia
-indistinct post margins
-asstd with bony defects
-may extend into infratemporal fossa or intracranially
*CT scan heterogenous well circumscribed mass
T/T –same
CAPILLARY HAEMANGIOMA-spot
- MC tum of orbit & periorbital area in childn
- Perinatal period but never at birth
SIGNS-
- Superficial strawberry naevus on lids
- Subcutaneous haemangioma
- Superior ant orbit MC inv-Dystopia
- Deep orb tum- UL eccentric proptosis without skin discolouration
- Haemangioma of the palpebral & forniceal conj-imp diag clue
- PULSATION & BRUIT ABSENT
CT SCAN-spot
- Homogenous soft tiss mass in ant orbit
- Extraconal mass with finger like posterior expansions
- No bony erosions
Grows upto 1 year & complete resolution by 7 years of age
SYSTEMIC ASSTN-
- High – output failure
- Kasabach-Meritt syn
- Maffuci syn
T/T-
IND-
- Amblyopia sec to induced astigmatism & anisometropia
- ON compression
- Exp KP
- Sev cosmetic blemish,necrosis & inf
T/T-
1.Steroid inj-Triamcinolone acetonide 40mg + Betamethasone 6mg into the lesion
-complications-retrograde forcing of sol into the CRA
-skin depigmentation & necrosis
-Blding
-Fat atrophy
2.Sys steroids
3.Local resection with a cutting cautery – reduces bulk of the tum-late & inactive stg
4.Low dose radiotherapy
CAVERNOUS HAEMANGIOMA-spot
- MC benign orb tum in adults
- F > m
- Most frequent within the ms cone behind the globe-axial proptosis
- 4th -5th decade
- Growth accelerated during pregnancy
SIGNS-
- Axial proptosis
- Gaze-evoked transient blurring of vision
- Optic disc edema
- Choroidal folds
CT SCAN-well-circumscribed retrobulbar mass with homogenous enhancement
T/T-
Surgical excision
Well-encapsulated,so easy to remove
PLEOMORPHIC LACRIMAL GLAND ADENOMA-patho spot
Benign mixed cell tum
- MC epithelial tum of the lacrimal gld
- Derived from ducts, stroma & myoepithelial elements
C/F-
- 5th decade
- Painless
- Slowly prog swelling in superolat part of orbit
- Swelling from orbital lobe-inferonasal dystopia
Smooth, firm & non-tender
- Posterior expansion-proptosis
-O’plegia
-choroidal folds
* swelling from palpebral lobe-does not displace the globe
CT SCAN-Mass indents the lacrimal bone but does not destroy it
T/T-
Surgical excision-
Palpebral lobe-Anterior orbitotomy
Orbital lobe-Lateral orbitotomy
Avoid a prior biopsy to prev seedling
LACRIMAL GLAND CARCINOMA-patho spot
HISTOLOGICAL TYPES-
- Adenoid-cystic
- Pleomorphic adenocarcinoma
- Mucoepidermoid
- Squamous cell ca
C/F-
- 4th -6th decade
- Pain
- Long-standing proptosis
- Sudden increase in size
- SIGNS-Mass in lacrimal gld area
-inferonasal dystopia
-post extension & superior orb fissure inv-conj &
Episcleral congn & O’plegia
-limited elev & abduction
-hypoaesthesia in area supplied by lacrimal N
-disc edema &choroidal folds
CT SCAN- Bone erosion & calcification
BIOPSY- No well-defined capsule
Neurological assessment is mandatory bcos adenoid cystic Ca spreads perineurally into cavernous sinus
T/T
1.Orbital Exenteration or mid-facial resection
2.Radiotherapy
OPTIC NERVE GLIOMA-spot
- Slow-growing pilocytic astrocytoma
- 1st decade
- Girls
- Neurofibromatosis-I
C/F-
- slowly prog visual loss
- proptosis next [Axial ] Since tum grows from inside out
SIGNS-
- ON head initially swollen,later atrophic [OA is MC than Papilloedema-VIVA]
- Optociliary shunt Vs
- RAPD
INV-
- CT scan-fusiform enlargement of ON
- MRI- shows intracranial extension to inv chiasma & hypothalamus
- X-RAY-Enlarged optic foramen
-Erosion of ant wall of sella & ant clinoid process-‘J’ shaped sella
GLIOBLASTOMA MULTIFORME-
Malignant optic glioma in adults
Painful visual loss
Death
T/T-
1.Observation if no e/o growth & visual loss→ Visual field tests
& MRI every 6-12mo to detect intracranial extension
2.If poor vision & increasing proptosis→Remove the lesion via a craniotomy & superior orbititomy
3.If intracranial extension→ RT & chemotherapy
VIVA-
Sudden increase in proptosis- Suggestive of malignant transformation.
OPTIC N SHEATH MENINGIOMA-spot
- Arise from meningothelial cells of arachnoid villi
- Middle-aged females
C/F-
Transient obscuration of vision-UL
SIGNS-
Classic triad-visual loss
-OA
-optociliary shunt Vs
- Optic N dysfunction & chronic disc edema→atrophy
- Optociliary shunt Vs
- Restrictive motility defects,in upgaze [d/t the tum splinting the ON]
- Proptosis [d/t intraconal spread] first. [ grows from out→ in]
INV-
- Ct scan-Tubular thickening & calcification of ON-“ TRAMTRACK “
T/T-
- Surgical excision
- Radiotherapy
- Stereotactic radiation therapy-gamma knife
CAVERNOUS SINUS THROMBOSIS [J-05,j-07-applied anat of CS]-spot
COMMUNICATIONS-diag from notes
- Anteriorly-Face→
-nose→
-PNS→ superior &inferior ophthalmic vein
-orbit→
2.Posteriorly→ middle ear→Sup & inf petrosal sinus
3.Superiorly→ meninges & cerebral abscess→middle meningeal veins
4.Inferiorly→ pterygoid venous plexus
5.Medially with each other thru transverse sinus
TRIBUTARIES-
A] FROM THE ORBIT-
1) Superior oph vein
2) Br of inferior oph vein
3)Central retinal vein
4) Medial ophthalmic vein
B] FROM THE BRAIN-
1) Superficial middle cerebral vein
2) Inferior cerebral vein
C]FROM THE MENINGES-
1) Sphenoparietal sinus
2) Middle meningeal vein
AETIO-
1/ Inf may occur via orbital veins as in-
* erysipelas
* septic lesions of face
* orbital cellulites
* inf of mouth,nose,ear.accessory sinuses
* metastasis in inf & septic conditions
* HZO
* mucormycosis
* dental inf
Acute inf-gram+ bact
Chronic inf-gram –ve bact & fungi
- Injudicious squeezing of furuncle on upper lip
- Tumours in the cavernous sinus-
-meningioma
-pituitary adenoma
-craniopharyngioma
-mets
4. Aseptic cavernous sinus thrombosis-
- Polycythemia
-sickle cell anaemia
-Trauma
-neurosurgery
-pregnancy
-OCP
C/F-Systemic-
- fever
- sev headache
- nausea & vomiting
- rigors
- altered sensorium
Ocular-
- initially UL but soon becomes bil
- sev supraorbital pain [oph div of V n]
- III, IV, VI n palsy [First sign-Paralysis of opp LR shud be carefully watched in any suspicious case of inf UL proptosis]
- Congestion of facial,conj, & retinal veins
- Motility def
- Pupils- immobile & dilated
- Cor –anaesthetic
- Proptosis-late onset & rapidly prog
- Diplopia
- Ptosis
- Oedema of mastoid reg-pathognomic sign
- CST + proptosis + disc swelling→sphenoid sinus dis
- CST + proptosis + disc swelling + oedema in mastoid reg →Thrombosis of emissary vein
T/T-
1.IV broad spectrum antibiotics
2.Analgesics
3.Anti-inflam drugs
4.Anticoagulants
RHABDOMYOSARCOMA-patho
- MC childhood prim orbital malignancy
- CELL TYPES-
- Embryonal-most favourable prog
→ Botyroid
→spindle cell
2.Alveolar-invades the orbit
-poor prog
3.Pleomorphic
C/F-
- Presents in the 1st decade [ avg- 7 yrs]
- Rapidly prog proptosis
- Sites-retrobulbar
-superior
-inferior
* palpable mass
* Ptosis
*swelling & inj of overlying skin but skin is not warm
* Parameningeal tum show bony destruction, LN dissemination & CNS inv
INV-
1.CT SCAN-Poorly defined mass of homogenous density
-bony destruction
2.For metastatic spread-
* chest x-ray
* LFT
* BM biopsy
* Lumbar puncture
MC sites for spread –lung & bone
T/T-
1.RT- 5000 rads for 5 weeks with weekly vincristine & cyclophosphamide.
After RT , Vin + cyc + doxorubicin 3/ week for 1 year or longer if metastasis
2.Chemotherapy-Vincristine
3.Surgical excision-For rare, recurrent & radioresistant tum
CRANIOSYNOSTOSIS
DEF- Group of disorders with premature fusion of cranial sutures & sev orbital abnormalities.
2 entities-
CROUZON’S SYNDROME
- premature fusion of coronal & sagittal sutures
- AD
- OCULAR-
- Shallow orbit [arrested growth of maxilla & zygoma]→ proptosis
- Hypertelorism [wide separation of orbits ]
- V-exotropia & hypertropia
- others-aniridia, blue sclera, cataract, ectopia lentis, glaucoma, coloboma, megalocornea, ON hypoplasia
SYSTEMIC-
- short AP head distance & wide cranium
- mid-facial hypoplasia
- ‘parrot-beak’ nose
- ‘frog-like’ facies
- Mandibular prognathism
- ‘Inverted V shaped palate
- Acanthosis nigricans
APERT SYNDROME
AD
OCULAR-
- Ectopia lentis
- Congenital glaucoma
- Shallow orbit
- Proptosis
- Hypertelorism
- Exotropia
- Anti-mongoloid slant
- OA
- Exp KP
- Keratoconus
SYSTEMIC-
- Oxycephaly with flat occiput & steep head
- Horizontal groove above supraorbital ridge
- Midfacial hypoplasia
- Parrot beak nose
- High arched palate
- Cleft palate
- Bifid uvula
- Syndactyly
- Anomalies-heart,lungs kidneys
- Mental retardn
ORBITOTOMY
SURGICAL ROUTES-
- Transcutaneous anterior O’tomy
- Medial transconjunctival O’tomy
- Lateral O’tomy
- Superior O’tomy-Domain of neurosurgeon
1.. TRANSCUTANEOUS ANTERIOR O’TOMY
IND-
To biopsy / excise small lesion located in anterior extraconal orbital space
INCISION-Upper lid crease to access the superior orbit or 2mm below the LL lash line to access the the inf orbit.
Orbicularis ms is opened→ orbital septum is cut→visible lesion biopsied /dissected→ bleeders cauterized & wound closed with sutures
2.MEDIAL TRANSCONJUNCTIVAL O’TOMY-
Ind-To access the anterior medial intraconal / extraconal orbital space for biopsy & tum removal
PROCEDURE-
Conj is cut ant to MR insertion→tenon’s capsule is separated→MR cut from its insertion→ globe rotated laterally→malleable retractors are used to visualize post tenon’s cap→opening of this layer gives access to retrobulbar space→tum is dissected→MR is reattached to the globe→ conj closed with sutures
LATERAL O’TOMY- [D-02]
IND-
- dermoid
- RB
- Rhabdomyosarcoma
- Pseudotum
- ON glioma
- Meningioma
- TED
- Cavernous haemangioma
- Lacrimal gld tum
- Melanoma
- BCC
Steps-
Temporalis ms is incised→periosteum is drilled for subsequent wiring→lateral orbital wall is removed →tum is excised→temporalis & periosteum are repaired
CHOROIDAL FOLDS-
- Idiopathic
- ON Glioma
- Meningioma
- Posterior scleritis
- TED
- Hypotony
ORBITAL EXENTERATION-
DEF-Removal of the entire eyeball & orbital contents along with the lids, EOM &orb. Fat.
IND-
- Sebaceous cell ca
- Malignant lacrimal gld tum
- Adv rhabdomyosarcoma
- Extensive fungal inf not responding to t/t
C/I- Metastasis
,
ORBITAL IMPLANTS[ d-04]
1] CORALLINE HYDROXYPATITE-
* Comprises of coral reef
* Becomes integrated as a part of recipient’s orbital tissue
* Biocompatible
* Forms a scaffolding for fibrovascular ingrowth
* Provides improved motility
* Less incidence of migration & extrusion
* Disadv-
- costly
-Wrapping material needed
-High rate of implant exposure
2] MEDPOR [ POROUS POLYETHYLENE]
* Synthetic plastic material
* Biocompatible
* Does not prov as complete a scaffold for fibrovascular ingrowth
* High tensile strength
* Smooth external surface
* No need of wrapping material.EO ms directly sutured onto the implant
* More economical
* can be used after a prim enucleation or evisceration or as a sec implant
*Low rate of implant exposure
WRAPPING MATERIALS-
- Sclera
- Fascia lata
- Polyglactin mesh-adv-Easy to use
-longer shelf-life
-no need for donor tiss
-less tissue reaction
No comments:
Post a Comment